










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkThe European Journal of Psychiatry
Print version ISSN 0213-6163
Eur. J. Psychiat. vol.25 n.3 Zaragoza Jul./Sep. 2011
https://dx.doi.org/10.4321/S0213-61632011000300005
Alcohol and drug dependence in adults with attention-deficit/hyperactivity disorder: Data from Germany
Martin D. Ohlmeier* **; Eva Goseberg*; Mandy Roy*; Wolfgang Dillo*; Andreas Kordon***; Vanessa Prox-Vagedes*
* Department of Psychiatry, Social Psychiatry and Psychotherapy, Hannover Medical School (MHH), Hanover, Germany
** Department of Psychiatry and Psychotherapy, Ludwig-Noll-Hospital, Klinikum Kassel Kassel, Germany
*** Department of Psychiatry and Psychotherapy, Medical University of Luebeck Luebeck, Germany
ABSTRACT
Background and Objectives: The objective of the present study was to obtain information about the prevalence of addiction disorders in ADHD patients in a German study population, to compare the prevalence of addiction disorders in ADHD patients to that in the normal population according to the German Epidemiological Addiction Survey, and to determine which drugs are consumed most by ADHD patients.
Participants: The sample consisted of 61 patients (average age 35.11 ± 9.33 years) from our ADHD consultation who were consecutively included in our study over a period of 12 months.
Measurements: We diagnosed ADHD according to DSM-IV-R and by assessing the WURS-k, CAARS and BROWN ADD scales. For diagnosing addiction we conducted the EuropASI, the IDCL, the QOD and the FTNA. For differential diagnosis we assessed the SCL-K.
Results: About half of our study population of ADHD patients were diagnosed with a dependence disorder (50.8%, n = 31). Twenty one dot three percent (n = 13) were suffering from an alcohol dependence, 13.1% (n = 8) from a substance use disorder (SUD) and 18% (n = 11) from a combination of both addictions. The drug consumed most commonly by ADHD patients was cannabis. Alcohol and substance abuse commenced significantly earlier in patients with ADHD than in patients with addiction disorders without comorbid ADHD.
Conclusions: Our data show that the risk of developing a dependence disorder is elevated in ADHD patients. Clinicians should bear in mind that the characteristics of a dependence in ADHD patients are clinically more pronounced and that an addiction in ADHD patients starts earlier than usually expected.
Key words: ADHD; Adults; Addiction; Epidemiology; Comorbidity.
Introduction
ADHD in adulthood
Attention-Deficit/Hyperactivity Disorder (ADHD) is the most frequent psychiatric disorder in childhood and adolescence1. According to a survey of the Robert Koch Institute (Berlin, Germany), the prevalence rate of ADHD in children and adolescents in Germany is 3.9%1. Epidemiological studies have shown that symptoms of childhood ADHD persist into adulthood in 30 to 80 percent of cases2. In a survey of the American population in 2006, a prevalence of 4.4% was ascertained for ADHD in adulthood3.
The disorder is over-represented in male subjects (3:1 to 4:1)4. This may be due to the fact that boys suffer more often from the hyperactive, impulsive subtype, which prompts parents to consult a physician5, whereas girls suffer more often from the inattentive subtype and are diagnosed more randomly or simply later in life1. These facts relativise the gender ratio in favour of the inattentive subtype with respect to DSM-IV6. According to the "German guidelines for ADHD in adulthood"7, there is no need to treat an adult with ADHD with medication right away. A treatment is indicated if the patients are suffering from ADHD symptoms strongly in one part of their lives or problems occur in different parts of their lives. There are manifold treatment options, e.g. pharmacological treatment or psychotherapy. In principle the therapy of an ADHD adult should be multimodal to comprise the comorbidities as well8. An early treatment of ADHD seems to be a protective factor against developing an SUD in later life9.
Substance use disorders
Substance use disorders (SUDs) are a heterogeneous disease pattern. The current theory about the pathogenesis of SUDs comprises a multimodal concept including physical, mental and social factors. SUD is diagnosed according to ICD-104 or DSM-IV-R10. The criteria for the diagnosis are similar to each other but differ in the point that DSM-IV also includes social and interpersonal factors11.
SUDs are a major social problem. In Germany, the most often diagnosed SUD is nicotine dependence, at 27% of the German population, divided into 85% regular users and 15% infrequent users12. The second most common SUD in Germany -especially in men- is alcohol consumption. According to DSM-IV, 2.4% of the population between the age of 18 and 65 years are diagnosed with alcohol dependence (3.4% men; 1.4% women). In absolute numbers, this means 1.3 million of the entire German population13. The data concerning substance abuse/SUD is harder to interpret, because the existing data do not differentiate between abuse and dependence. In the year 2000, 0.9% of the German population between the age of 18 and 59 were diagnosed with an abuse/dependence (1-year prevalence). This means in absolute numbers that there are 290,000 addicted people in the entire German population with at least one diagnosis of addiction according to DSM-IV14. Data from the year 2007 for the prevalence of the different substances used throughout life (according to the "epidemiological addiction survey") show that cannabis is the most commonly consumed illegal substance, at 24.7% of drug consumers in the year 2006. It is followed by amphetamines (2.7%) and cocaine (2.7%)15,16.
Comorbidity of ADHD and alcohol and substance use disorders
The relationship between ADHD and SUD has become increasingly important17-21. In general, ADHD patients are said to have twice as high a lifetime risk of developing an SUD17. Various studies have reported an elevated comorbidity of ADHD and SUD in 45% to 70 %22-24. Biederman and colleagues found a higher rate (44%) of comorbid alcohol abuse/addiction in 239 adult ADHD patients, in contrast to 268 non-ADHD adults with a comorbid alcohol abuse/addiction of 24%18. Similar comorbidity rates were found by Shekim and colleagues (34%)25 and Downey et al. (33.3%)26. In one of our previous study populations, we diagnosed ADHD in 20.9% to 33.3% of alcohol addicted patients, which is consistent with the figures found in US-American studies27,28. In a review article, Wilens and others showed that the coherence between SUD and ADHD is strong, too29. Various studies about alcohol and substance abuse have shown that 15-25% of adults with a dependence disorder fulfil the diagnostic criteria of ADHD29-32. The most popular drug in ADHD patients seems to be cannabis, with a comorbidity rate of 21%17,28,33. A comorbidity rate of cocaine addiction and ADHD was found in 11% to 35% of the patients30,33,34. Also the symptoms of addiction start earlier in these patients and the course of the disease is worse than in cocaine addicted patients without ADHD30.
Early pharmacotherapy in children with ADHD seems to be a factor protecting against the development of an SUD in later life35,36. Metaanalysis37 as well as animal models38-40 indicate that early treatment may be effective in avoiding substance abuse. 20-day-old rats -similar to childhood in mankind- with symptoms of hyperactivity showed a diminished interest in cocaine after being treated with stimulants38,39.
The risk of developing nicotine dependence seems also to be elevated in ADHD patients in a US-study, with a prevalence rate of about 40%41. These figures are significantly higher than that of the general US-population, at 27%. Adolescent ADHD patients have twice as high a risk of developing a nicotine dependence as adolescents without ADHD, in whom cigarette smoking is a further risk factor for developing a subsequent substance dependence42. The coincidence of an addiction to nicotine in adults with ADHD was 40-75% in a US-American study (vs 19-26% in the normal population)41.
Biederman and colleagues demonstrated that untreated ADHD is a risk factor for the development of an SUD35. The groups of Faraone43 and Wilens37 drew the conclusion that a pharmacological treatment had no negative influence on SUDs in ADHD patients. In contrast, various studies have shown that a treatment of addicted ADHD patients with stimulants reduces drug consumption and "craving"31,37,44,45. Adolescents medicated with stimulants showed a lower risk of developing an addiction (cocaine, alcohol and other drugs)35.
In our own studies27,28, we demonstrated that many substance-dependent patients suffer from an -often not diagnosed- ADHD. Within the scope of these studies, 91 patients with alcohol dependence and 61 patients with multiple substance dependence were examined for the presentation of ADHD. 23.1% of the alcohol-dependent patients showed evidence of retrospective ADHD affliction in childhood. In the group of substance-addicted patients, 54.1% presented with diagnostic criteria for ADHD in childhood. In addition, in both groups examined, it was shown that a comorbid ADHD supported earlier first consumption of alcohol or substances28. Studies of other groups focused on coherences between different subtypes of adult ADHD patients with regard to psychosocial adjustments, personality traits and other psychiatric comorbidities46,47.
Aims of the study
The aim of this study was to identify the prevalence of SUD in ADHD adults of our specialised ADHD consultation in the German population. Several studies have been conducted in the USA, but data from Germany are lacking. We wanted to compare the prevalence of the comorbidity of ADHD and SUD with the data of the German population. Another aim was to determine which substances are most commonly consumed and to establish the characteristics of substance dependence in ADHD adults, e.g. whether ADHD adults start consuming drugs earlier in life or whether the course of addiction in ADHD patients is more aggressive.
Subjects and Methods
61 adult patients (28 males, 33 females - average age 35.11 ± 9.33 years) were enrolled in this study. In aiming to find out about the prevalence of ADHD patients who are suffering from a comorbid dependence disorder, we recruited all patients consecutively who presented at our ADHD consultation and were diagnosed with ADHD (diagnostic criteria of DSM-IV-R) over a period of 12 months. Only two patients refused to take part in our study. Every participating patient gave written consent to participate in our study. The minimum age had to be 18 years.
Excluded from the study were patients with acute psychoses and people who were impaired by their illness to such an extent that they were not able to take care of their personal needs. Other comorbid illnesses such as major depression were acknowledged but did not lead to exclusion from the study. To screen for relevant comorbid diagnoses the IDCL and the SCL-90-R were conducted48,49.
For retrospective assessment of childhood ADHD, the DSM-IV-R symptom checklist for ADHD50 was used, as well as the authorised German translation of the Wender Utah Rating Scale (WURS-k)51.
Moreover, the individuals were divided into diagnostic subgroups of ADHD as the inattentive type (DSM-IV-R: 314.00, according to ICD-10: F98.8), hyperactive-impulsive type (DSM-IV-R: 314.01, according to ICD-10: F90.1) and combined type (DSM-IV-R: 314.01, according to ICD-10: F90.0). The Conners Adult ADHD Rating Scales (CAARS, long version)52 were used to assess the persisting symptoms of ADHD in adults. Also the Brown Attention Deficit Scales53 were applied. Every patient was finally diagnosed by a specially trained psychiatrist who conducted a semi-structured clinical interview with each patient according to criteria of DSM-IV-R.
The patients who had been diagnosed with ADHD were then screened for a possible diagnosis of a substance dependence or an alcohol dependence according to diagnostic criteria of DSM-IV-R and ICD-10. The "Internationale Diagnosen Checkliste für ICD-10" (IDCL) was conducted to validate the clinical diagnosis49,54. The European Addiction Severity Index (Europ-ASI)55 was used for evaluation of the addiction case history. To evaluate the characteristics of a given dependence in more detail, a questionnaire concerning alcohol and drug addiction (QOD) was also conducted56. Nicotine consumption was tested using the Fagerström Test of Nicotine Dependence57 and then graded into 'minimal', 'average' or 'high' nicotine dependence.
Approval for this study was given by the Ethics Committee of Hannover Medical School.
Statistical Analysis
Statistical analysis was conducted with the SPSS program (version 15.0, SPSS Inc., Chicago, IL). The chi-square test was performed for comparison of proportions. The level of significance was p < 0.05. Comparison of means were conducted using single factor analysis of variance (ANOVA). Post-hoc analyses were calculated using the Scheffé test.The assessment of homogeneity of variances was guaranteed using the Levene test.
Results
According to DSM-IV-R and ICD-10, 61 patients fulfilled the required diagnostic criteria of ADHD and were definitely suffering from ADHD. The group was composed of 28 male (45.9%) and 33 female (54.1%) patients with an average age of 35.11 ± 9.33 years. The sociodemographic data are presented in Table 1.

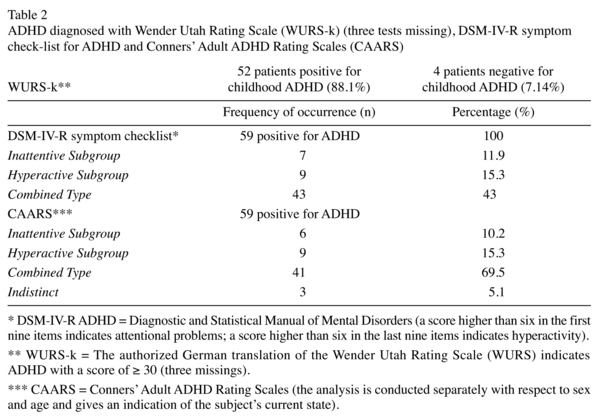
52 (88.1 %) of the 61 patients achieved the cut-off of 30 or more points in the WURS-k and therefore fulfilled the criteria for ADHD symptoms in childhood. The DSM-IV-R symptom checklist retrospectively confirmed the ADHD diagnosis in childhood in 59 patients (96.2 %). The CAARS gave evidence of persisting ADHD in adulthood in all 59 patients, too. Two of the 61 patients could only be diagnosed with ADHD according to the interview of an experienced and specially trained physician, so that they were excluded from the diagnostic differentiation of the ADHD subtypes. According to DSM-IV-R, 9 patients (15.3%) were categorized as 'hyperactive type', 7 (11.9%) as 'inattentive type' and 43 (72.9%) as 'combined type' of ADHD. The same differentiation was conducted using the CAARS. The categorization showed similar results. The data concerning the diagnosis of ADHD and the subtypes are presented in Table 2.
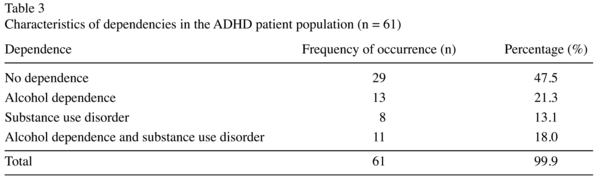
Approximately half of the patients (50.8%) diagnosed with ADHD were suffering from a comorbid active or remitted dependency according to the IDCL. 21.3% of the patients (n = 13) were diagnosed with an alcohol dependency, 13.1% with an SUD (n = 8) and 18% with a comorbid alcohol and SUD (n = 11). The data are presented in Table 3.
Alcohol
29.5% (n = 18) of our ADHD patients could be diagnosed with an alcohol dependency according to IDCL. The average age of first alcohol consumption was 13.97 years (± 3.27). The first alcohol excess was 15.09 (± 2.94) years according to the QOD. A frequent consumption of three times a week was started at the age of 19 (± 4.94) years.
Substances
With the aid of the IDCL, 31.1% (n = 19) of the patients could be diagnosed as suffering from a substance dependence, including three cases with a reasonable suspicion. In 68.4% of the cases (n = 13) the symptoms were remitted.
Cannabis was the substance most commonly consumed, at 29.5% of the whole population according to EuropASI and QOD. This means that 94.7% of the substance dependent ADHD patients in our study consumed cannabis over a period of 8 ± 7.58 years. The start of the frequent consumption of cannabis was 17.68 years ± 4.22. Hence, cannabis was the first illegal drug to be consumed regularly.
For a detailed description of the substances consumed see Table 4.

The majority of the substance dependent ADHD patients abused multiple drugs (73.7%, n = 14), starting at an age of 17.88 (± 7.78) years. This multiple substance dependence was due to the use of cannabis (94.73%, n = 18), amphetamines (47.36%, n = 9), cocaine (36.84%, n = 7) and hallucinogens (36.84%, n = 7).
Nicotine
According to the Fagerström test (FTNA), there was no nicotine dependence in 53.3% of the patients at the time of the interview. In 11.6% (n = 7) the dependence was classified as "very low", 10% (n = 6) as "low", 5% as "middle" and 20% as "extreme".
Discussion
The prevalence of an addictive disorder seems to be elevated in ADHD adults, as approximately every second ADHD patient (50.8%) in our study was suffering from an addictive disorder.
These results are similar to those of Jacob et al.22, who found a lifetime prevalence of a comorbid SUD in 45% in a large German cohort study. Similarly, Wilens and colleagues24 found a comorbidity of ADHD and alcohol or substance use dependency in 71%. These results support the theory that ADHD patients are at high risk of developing addictive disorders.
Our study population revealed an addiction to alcohol in 39.3%. This prevalence rate includes both current and remitted cases of alcohol addiction, which complicates a direct comparison with the prevalence rate of alcohol dependence in the normal population. Nevertheless, the number of alcohol dependent patients with ADHD seems to be elevated in comparison to the normal German population. According to evaluations of German society for addiction ("Deutsche Hauptstelle für Suchtfragen e.V. (DHS)"), 2.4% of the German population between the age of 18 and 64 years are addicted to alcohol according to DSM-IV criteria13.
Studies by Biederman and colleagues18 and Wilens29 found similar rates for this comorbidity, with 44% alcohol addicted ADHD patients. Also Downey et al.26 and Shekim et al.25 describe a comorbidity of alcohol dependency and ADHD in 34% of the patients. Regarding these results, our data seem to be realistic and support the theory that the prevalence of alcohol dependence is elevated in ADHD patients.
The numbers of ADHD patients with a multiple SUD show that ADHD patients also have a higher risk of becoming addicted to illegal drugs. 14.2% of the German population try an illegal drug at least once in their lives60. Compared with our prevalence rate of 31.1% substance abusing ADHD patients, the lifetime risk of consuming drugs is twice as high. In contrast to the alcohol addiction data, these figures can be compared because the statistics of the normal population include both current drug consumption and consumption during the past, and also considers cannabis as an illegal drug. Wilens29 found a similarly elevated rate for psychoactive SUD in ADHD patients, at 9% to 30%. The research groups of Mannuzza23 and Biederman61 even found a percentage rate of about 50%. Our results are therefore in line with the hypothesis that ADHD is a risk factor for addiction to illegal drugs17 which means that ADHD patients have also a higher risk of getting in conflict with the law.
Taking a closer look at the alcohol consumption habits of the adult ADHD patients in comparison to the normal population, we were unable to find any differences concerning first alcohol consumption or first intoxication with alcohol. The mean age of first alcohol consumption of our ADHD patient group was 13.97 (± 3.27) years. The mean age of first intoxication was 15.09 (± 2.94) years. In the normal population, alcohol is first consumed at 12.8 years and the critical level of alcohol first exceeded at 13.8 years62. It is certainly difficult to compare our study group with the youth of today, because the trend is for alcohol to be started earlier than when our patients were teenagers. Comparison of an older normal population might have shown a difference in first alcohol consumption. This result was nonetheless unexpected, because various authors have described an earlier start and a more aggressive form of SUD in patients with ADHD24,32.
Whereas the first symptoms of alcohol dependence can be recognized earlier in ADHD patients than in the normal population, our patients reported the first symptoms of alcohol dependence at the age of 22.43 (± 5.47) years. This finding is consistent with the work of Wilens and colleagues24, who found that the career of dependence starts approximately three years earlier in ADHD patients in comparison to the normal population. Similar results were reported by Johann and colleagues63. Within their study including 314 patients with and without ADHD, they arrived at the conclusion that ADHD patients become addicted to alcohol significantly earlier (24 instead of 30 years).
The group of Wilens24 found that patients with ADHD also develop a dependence to psychoactive substances around three years earlier in contrast to people without ADHD. In general ADHD patients seem to change earlier and faster from a substance abuse into an addictive disorder than patients without ADHD64. Even if there is no difference between ADHD patients and the normal population with respect to first alcohol consumption, the clinician should bear in mind that the risk of ADHD patients developing an addiction is higher if they are already abusing substances.
The illegal substance most frequently consumed was clearly cannabis. Regular consumption was started at 17.68 (± 4.22) years. These results are congruent with the study of Wilens29, who described the first consumption of cannabis typically at an age between 17 and 19. 29.5% of our study population consumed cannabis regularly. This is in line with the findings of Tzelepis and colleagues33, who found a prevalence of regular cannabis consumption in their study population of 21%. In a multi-centre study, Tims and colleagues65 found that ADHD is the second most common comorbidity in adolescents who abuse cannabis, at 38%. Cannabis consumption may be a kind of "self-medication" for ADHD patients. The "self-medication hypothesis" of the dependence disorders was postulated in 1985 by Khantzian66. The core statement of the hypothesis is that people who develop a substance dependence are already suffering from other psychiatric symptoms, such as anxiety disorders or depression, but also hyperactivity. Khantzian developed the hypothesis that each drug consumer unconsciously selects the drug that reduces the symptoms from which he is suffering most. The preferred substances to be consumed by ADHD patients are according to Khantzian the group of the amphetamines as well as cocaine, because ADHD patients describe commonly reassuring effects after consumption of the above mentioned substances - at first sight, apparently a "paradoxical" reaction66,67. In a study published recently, Pandolfo and colleagues68 reported that hyperactive adult rats show a significant influence in their behaviour after consumption of can-nabinoid substances in contrast to healthy rats, which supports the theory of self-medication of ADHD patients with cannabis.
Also the risk of developing a cocaine dependence seems to be higher in ADHD patients. We found a cocaine dependency in 14.8% of our patients. These figures are definitely higher than the prevalence in the normal population, which is 2.7% in Germany. Comparable percentages (11%) of the prevalence of cannabis dependence were described by Tzelepis et al.33. Conversely, Rounsaville and colleagues69 found positive criteria for childhood ADHD in 35% of cocaine abusing patients.
Concerning nicotine dependence, we observed another highly prevalent comorbidity in ADHD patients (45.9%), which is almost twice as high as the nicotine dependence in the normal population, at 27%. Similarly, Pomerleau and colleagues41 found a prevalence rate of nicotine dependence of 40-75% in ADHD patients. Nicotine consumption may also be a kind of "self-medication", as Lambert and Hartsough70 found tobacco consumption to be twice as high in ADHD adults. This hypothesis is underlined by Wilens et al.71, who described that more than one third of ADHD adolescents and adults use nicotine for "self-medication" which is according to the theory of Khantzian72,73. The high prevalence of nicotine dependence in ADHD patients can be explained pathophysiologically by the fact that nicotine stimulates the release of neurotransmitters (e.g. acetylcholine, dopamine and serotonin) and, accordingly, the attention span is increased. Nicotine appears to have an effect on the nucleus accumbens similar to that of the amphetamine derivatives74. Some studies support the hypothesis that nicotine can be used therapeutically in ADHD patients75,76.
Several SPECT studies have shown evidence of a comparable effect of nicotine on the dopamine transporter (DAT), known also with methylphenidate77. A marked decrease of striatal DAT has been observed in nicotine-dependent ADHD patients78. It is of particular interest to note that various dopaminergically and noradrenergically effective drugs, such as bupropione, nortriptylene and moclobemide, are effective and beneficial in both the treatment of nicotine dependence and in ADHD45.
Other reasons for the high vulnerability of SUD in ADHD patients might also be the typical impulsivity, such as the readiness to take risks and a form of "sensation seeking" behaviour. The concept of "sensation seeking" appeared for the first time at the end of the 1970s79,80. The basis for this new concept was the observation that some people show a stronger desire for new attractions and are ready to take higher risks to achieve a stimulation by new attractions. There also appeared to be a positive correlation between impulsiveness and "sensation-seeking behaviour", which was discussed for the purposes of a biological mechanism81. Cloninger interprets "curiosity behaviour" as an expression of a low basal dopaminergic activity. With the help of positron emission tomography (PET) and single photon emission computed tomography (SPECT), controlled proof of a raised dopamine-transporter density in the striatum -a disturbance of dopaminergic function- leads to the assumption that ADHD patients have a strong "curiosity behaviour" in the narrower sense77,82,83. The reduced dopamine level in ADHD patients may therefore explain the strong "novelty seeking", which would explain the raised impulsiveness and risk seeking behaviour, on the one hand, and the higher risk concerning substance dependence, on the other. Verheul and others (2001)58 come to similar results in their study. They describe that some personality traits seem to be associated with the development of an SUD, such as impulsivity, hyperactivity and "sensation seeking". Also from the point of view of genetics there seems to be evidence that there is coherence between ADHD and SUD. Comorbidity of alcoholism and ADHD forms a distinct phenotype that contributes substantially to the so-called type 2 alcoholics according Cloninger. A genome-wide association (GWA) study with pooled DNA in adult ADHD employing approximately 500K SNP markers identifies novel risk genes and reveals remarkable overlap with findings from recent GWA scans in SUDs59.
Limitations
One general problem in prevalence studies is that not every patient wants to take part in a study. As mentioned above two patients refused to take part in the study. This can falsify the results. Enough patients participated in our study for conclusions to be drawn, but the patients who did not agree to take part might have led to slightly different figures. Overall we must admit that 61 patients are not a very high number of patients.
Another problem is the work with self-assessment scales, which includes the risk that patients do not remember events in their past accurately and tend to affirm questions. We tried to reduce these risks by conducting a semi-standardized interview by an experienced clinician.
Conclusions
Our data show that the risk of developing a dependence disorder is elevated in ADHD patients. Clinicians should bear in mind that the characteristic of a dependence in ADHD patients is clinically more pronounced and that an addiction in ADHD patients starts earlier than one might possibly expect. The results of our study and clinical experience also indicate the importance of an early diagnosis and treatment of ADHD, i.e. a 'multimodal therapy' using pharmacological and psychotherapeutic concepts, which may help in reducing the onset and exacerbation of addictive illnesses.
Acknowledgments
The authors of this paper do not have any commercial associations that might pose a conflict of interest in connection with this manuscript. The authors thank all co-workers for their assistance in this study, particularly since no financial support was available.
Reference List
1. Huss M. Vorbereitung der Erhebung und Auswertung zur Prävalenz des Aufmerksamkeit-Defizit-Hyperaktivitäts-Syndroms (ADHS) in Deutschland im Rahmen des Kinder- und Jungend-Surveys des Robert-Koch-Instituts. Abschlussbericht an das Bundesministerium für Gesundheit und soziale Sicherung (BMGS). Bonn: 2004. [ Links ]
2. Barkley RA. Advancing age, declining ADHD. Am J Psychiatry 1997; 154: 1323-1325. [ Links ]
3. Kessler RC, Adler L, Barkley R, Biederman J, Conners CK, Demler O, et al. The prevalence and correlates of adult ADHD in the United States: results from the National Comorbidity Survey Replication. Am J Psychiatry 2006; 163: 716-723. [ Links ]
4. World Health Organization. Division of Mental Health, ICD-10. Geneva; 1990. [ Links ]
5. Weiss M, Hechtmann L, Weiss G. ADHD in adulthood. A guide to current theory, diagnosis and treatment. Baltimore: The Johns Hopkins University Press; 1999. [ Links ]
6. Wender PH, Wolf LE, Wasserstein J. Adults with ADHD. An overview. Ann N Y Acad Sci 2001; 931: 1-16. [ Links ]
7. Ebert D, Krause J, Roth-Sackenheim C. ADHD in adulthood-guidelines based on expert consensus with DGPPN support. Nervenarzt 2003; 74: 939-946. [ Links ]
8. Krause KH, Krause J, Trott GE. Hyperkinetic syndrome (attention deficit-/hyperactivity disorder) in adulthood. Nervenarzt 1998; 69: 543-556. [ Links ]
9. Wilens TE, Faraone SV, Biederman J, Gunawardene S. Does stimulant therapy of attention-deficit/hyperactivity disorder beget later substance abuse? A meta-analytic review of the literature. Pediatrics 2003; 111: 179-185. [ Links ]
10. American Psychiatric Association. DSM-IV-R Diagnostic criteria of the attention deficit-/hyperactivity disorder. Washington, DC; 2000. [ Links ]
11. Schuckit MA, Hesselbrock V, Tipp J, Anthenelli R, Bucholz K, Radziminski S. A comparison of DSM-III-R, DSM-IV and ICD-10 substance use disorders diagnoses in 1922 men and women subjects in the COGA study. Collaborative Study on the Genetics of Alcoholism. Addiction 1994; 89: 1629-1638. [ Links ]
12. Statistisches Bundesamt. Leben in Deutschland - Haushalte, Familien und Gesundheit. Ergebnisse des Mikrozensus 2005. Wiesbaden: Statistisches Bundesamt; 2006. [ Links ]
13. Hüllinghorst R., Kaldewei D., Lindemann F. Jahrbuch Sucht 2007, Epidemiologischer Suchtsurvey 2006. In: Sucht - Zeitschrift für Wissenschaft und Praxis, ed. Deutsche Haupstelle für Suchtfragen e.V. (DHS). 2006. [ Links ]
14. Hüllinghorst R., Kaldewei D., Lindemann F. Repräsentativerhebung zum Gebrauch psychoaktiver Substanzen bei Erwachsenen in Deutschland. 2000. [ Links ]
15. Kraus L, Pfeiffer-Gerschel T, Stonner T. Epidemiologischer Suchtsurvey 2006. Repräsentativerhebung zum Gebrauch und Missbrauch psychoaktiver Substanzen bei Erwachsenen in Deutschland. Sucht 2008; 54: 1-63. [ Links ]
16. BZgA 2007. Die Drogenaffinität Jugendlicher in der Bundesrepublik Deutschland 2004 (DAS). Version: Illegale Drogen, http://www.bzga.de/bot 2007; Seite 1417-html, Abruf: 15.08.2007. [ Links ]
17. Biederman J, Wilens T, Mick E, Milberger S, Spencer TJ, Faraone SV. Psychoactive substance use disorders in adults with attention deficit hyperactivity disorder (ADHD): effects of ADHD and psychiatric comorbidity. Am J Psychiatry 1995; 152: 1652-1658. [ Links ]
18. Biederman J, Wilens TE, Mick E, Faraone SV, Spencer T. Does attention-deficit hyperactivity disorder impact the developmental course of drug and alcohol abuse and dependence? Biol Psychiatry 1998; 44: 269-273. [ Links ]
19. Clure C, Brady KT, Saladin ME, Johnson D, Waid R, Rittenbury M. Attention-deficit/hyperactivity disorder and substance use: Symptom pattern and drug choice. Am J Drug Alcohol Abuse 1999; 25: 441-448. [ Links ]
20. Robbins TW. ADHD and addiction. Nat Med 2002; 8: 24-25. [ Links ]
21. Wilson JJ, Levin FR. Attention deficit hyperactivity disorder (ADHD) and substance use disorders. Curr Psychiatry Rep 2001; 3: 497-506. [ Links ]
22. Jacob CP, Romanos J, Dempfle A, Heine M, Windemuth-Kieselbach C, Kruse A, et al. Co-morbidity of adult attention-deficit/hyperactivity disorder with focus on personality traits and related disorders in a tertiary referral center. Eur Arch Psychiatry Clin Neurosci 2007; 257: 309-317. [ Links ]
23. Mannuzza S, Klein RG, Bessler A, Malloy P, LaPadula M. Adult outcome of hyperactive boys. Educational achievement, occupational rank, and psychiatric status. Arch Gen Psychiatry 1993; 50: 565-576. [ Links ]
24. Wilens TE, Biederman J, Mick E, Faraone SV, Spencer T. Attention deficit hyperactivity disorder (ADHD) is associated with early onset substance use disorders. J Nerv Ment Dis 1997; 185: 475-482. [ Links ]
25. Shekim WO, Asarnow RF, Hess E, Zaucha K, Wheeler N. A clinical and demographic profile of a sample of adults with attention deficit hyperactivity disorder, residual state. Compr Psychiatry 1990; 31: 416-425. [ Links ]
26. Downey KK, Stelson FW, Pomerleau OF, Giordani B. Adult attention deficit hyperactivity disorder: Psychological test profiles in a clinical population. J Nerv Ment Dis 1997; 185: 32-38. [ Links ]
27. Ohlmeier MD, Peters K, Kordon A, Seifert J, Wildt BT, Wiese B, et al. Nicotine and alcohol dependence in patients with comorbid attention-deficit/hyperactivity disorder (ADHD). Alcohol Alcohol 2007; 42: 539-543. [ Links ]
28. Ohlmeier MD, Peters K, Te Wildt BT, Zedler M, Ziegenbein M, Wiese B, et al. Comorbidity of alcohol and substance dependence with attention-deficit/hyperactivity disorder (ADHD). Alcohol Alcohol 2008; 43: 300-304. [ Links ]
29. Wilens TE. Attention-deficit/hyperactivity disorder and the substance use disorders: The nature of the relationship, subtypes at risk, and treatment issues. Psychiatr Clin North Am 2004; 27: 283-301. [ Links ]
30. Carroll KM, Rounsaville BJ. History and significance of childhood attention deficit disorder in treatment-seeking cocaine abusers. Compr Psychiatry 1993; 34: 75-82. [ Links ]
31. Levin FR, Evans SM, Kleber HD. Prevalence of adult attention-deficit hyperactivity disorder among cocaine abusers seeking treatment. Drug Alcohol Depend 1998; 52: 15-25. [ Links ]
32. Schubiner H, Tzelepis A, Milberger S, Lockhart N, Kruger M, Kelley BJ, et al. Prevalence of attention-deficit/hyperactivity disorder and conduct disorder among substance abusers. J Clin Psychiatry 2000; 61: 244-251. [ Links ]
33. Tzelepis A, Schubiner H, Warbusse LH, Nadeau K. Differential diagnosis and psychiatric comorbidity patterns in adult attention deficit disorder. New York: Brunner/ Mazel; 1995. [ Links ]
34. Volkow ND, Wang GJ, Ma Y, Fowler JS, Zhu W, Maynard L, et al. Expectation enhances the regional brain metabolic and the reinforcing effects of stimulants in cocaine abusers. J Neurosci 2003; 23: 11461-11468. [ Links ]
35. Biederman J, Wilens T, Mick E, Spencer T, Faraone SV. Pharmacotherapy of attention-deficit/hyperactivity disorder reduces risk for substance use disorder. Pediatrics 1999; 104: e20. [ Links ]
36. Huss M, Lehmkuhl U. Methylphenidate and substance abuse: A review of pharmacology, animal, and clinical studies. J Atten Disord 2002; 6 (Suppl 1): S65-S71. [ Links ]
37. Wilens TE, Faraone SV, Biederman J, Gunawardene S. Does stimulant therapy of attention-deficit/hyperactivity disorder beget later substance abuse? A meta-analytic review of the literature. Pediatrics 2003; 111: 179-185. [ Links ]
38. Andersen SL, Arvanitogiannis A, Pliakas AM, LeBlanc C, Carlezon WA, Jr. Altered responsiveness to cocaine in rats exposed to methylphenidate during development. Nat Neurosci 2002; 5: 13-14. [ Links ]
39. Brandon CL, Marinelli M, Baker LK, White FJ. Enhanced reactivity and vulnerability to cocaine following methylphenidate treatment in adolescent rats. Neuropsychopharmacology 2001; 25: 651-661. [ Links ]
40. Augustyniak PN, Kourrich S, Rezazadeh SM, Stewart J, Arvanitogiannis A. Differential behavioral and neurochemical effects of cocaine after early exposure to methylphenidate in an animal model of attention deficit hyperactivity disorder. Behav Brain Res 2006; 167: 379-382. [ Links ]
41. Pomerleau OF, Downey KK, Stelson FW, Pomerleau CS. Cigarette smoking in adult patients diagnosed with attention deficit hyperactivity disorder. J Subst Abuse 1995; 7: 373-378. [ Links ]
42. Wilens TE, Upadhyaya HP. Impact of substance use disorder on ADHD and its treatment. J Clin Psychiatry 2007; 68: e20. [ Links ]
43. Faraone SV, Biederman J, Wilens TE, Adamson J. A naturalistic study of the effects of pharmacotherapy on substance use disorders among ADHD adults. Psychol Med 2007; 37: 1743-1752. [ Links ]
44. Levin FR, Evans SM, McDowell DM, Kleber HD. Methylphenidate treatment for cocaine abusers with adult attention-deficit/hyperactivity disorder: A pilot study. J Clin Psychiatry 1998; 59: 300-305. [ Links ]
45. Riggs PD, Leon SL, Mikulich SK, Pottle LC. An open trial of bupropion for ADHD in adolescents with substance use disorders and conduct disorder. J Am Acad Child Adolesc Psychiatry 1998; 37: 1271-1278. [ Links ]
46. Sobanski E, Bruggemann D, Alm B, Kern S, Philipsen A, Schmalzried H, et al. Subtype differences in adults with attention-deficit/hyperactivity disorder (ADHD) with regard to ADHD-symptoms, psychiatric comorbidity and psychosocial adjustment. Eur Psychiatry 2008; 23: 142-149. [ Links ]
47. Jacob CP, Romanos J, Dempfle A, Heine M, Windemuth-Kieselbach C, Kruse A, et al. Co-morbidity of adult attention-deficit/hyperactivity disorder with focus on personality traits and related disorders in a tertiary referral center. Eur Arch Psychiatry Clin Neurosci 2007; 257: 309-317. [ Links ]
48. Franke G. SCL-90-R-Symptom-Checkliste. Göttingen: Beltz Test GmbH; 2002. [ Links ]
49. Hiller W, Zaudig M, Mombour W. IDCL Internationale Diagnosen Checkliste für ICD-10. Bern: Huber; 1995. [ Links ]
50. American Psychiatric Association. DSM-IV Diagnostic criteria of the attention deficit-/hyperactivity disorder. Washington, DC; 1994. [ Links ]
51. Retz-Junginger P, Retz W, Blocher D, Weijers HG, Trott GE, Wender PH, et al. Wender Utah rating scale. The short-version for the assessment of the attention-deficit hyperactivity disorder in adults. Nervenarzt 2002; 73: 830-838. [ Links ]
52. Conners CK, Erhardt D, Sparrow E. Conners' Adult ADHD Rating Scales (CAARS); 1999. [ Links ]
53. Brown TE. Brown Attention Deficit Disorder Scales. San Antonio: The Psychological Association. TX; 1996. [ Links ]
54. Hiller W, Zaudig M, Mombour W. Development of diagnostic checklists for use in routine clinical care. A guideline designed to assess DSM-III-R diagnoses. Arch Gen Psychiatry 1990; 47: 782-784. [ Links ]
55. Gsellhofer B, Küfner H, Vogt M. European Addiction Severity Index- Euro, nach der 5. Aufl. der amerika-nischen Version von McLellan und der europäischen Version des ASI; Manual für Training und Durchführung. Hohengehren: Schneider; 1999. [ Links ]
56. Driessen M, Schulte S, Wulff H, Sutmann F, Schaefer I. Diagnostische Aspekte bei Trauma und Substanzabhängigkeit. Stuttgart: Klett-Cotta; 2006. [ Links ]
57. Fagerstrom KO, Schneider NG. Measuring nicotine dependence: A review of the Fagerstrom Tolerance Questionnaire. J Behav Med 1989; 12: 159-182. [ Links ]
58. Verheul R. Co-morbidity of personality disorders in individuals with substance use disorders. Eur Psychiatry 2001; 16: 274-282. [ Links ]
59. Lesch KP, Timmesfeld N, Renner TJ, Halperin R, Roser C, Nguyen TT, et al. Molecular genetics of adult ADHD: converging evidence from genome-wide association and extended pedigree linkage studies. J Neural Transm 2008; 115: 1573-1585. [ Links ]
60. Kraus L, Bauernfein R. Repräsentativerhebung zum Gebrauch psychoaktiver Substanzen bei Erwachsenen in Deutschland 1997. Sucht 1998; 44 (Sonderheft 1): 3-82. [ Links ]
61. Biederman J, Faraone SV, Spencer T, Wilens T, Norman D, Lapey KA, et al. Patterns of psychiatric comorbidity, cognition, and psychosocial functioning in adults with attention deficit hyperactivity disorder. Am J Psychiatry 1993; 150: 1792-1798. [ Links ]
62. Richter M, Hurrelmann K. Jugend und Drogen Eine Studie zum wachsenden Bedarf an jungenspezischer Suchtprävention. Blickpunkt DER MANN 2004; 2: 6-10. [ Links ]
63. Johann M, Bobbe G, Laufkotter R, Lange K, Wodarz N. Attention-deficit hyperactivity disorder and alcohol dependence: a risk constellation. Psychiatr Prax 2004; 31 (Suppl 1): S102-S104. [ Links ]
64. Wilens TE, Biederman J, Mick E. Does ADHD affect the course of substance abuse? Findings from a sample of adults with and without ADHD. Am J Addict 1998; 7: 156-163. [ Links ]
65. Tims FM, Dennis ML, Hamilton N, Buchan J, Diamond G, Funk R, et al. Characteristics and problems of 600 adolescent cannabis abusers in outpatient treatment. Addiction 2002; 97 Suppl 1: 46-57. [ Links ]
66. Khantzian EJ. The self-medication hypothesis of addictive disorders: Focus on heroin and cocaine dependence. Am J Psychiatry 1985; 142: 1259-1264. [ Links ]
67. Khantzian EJ. An extreme case of cocaine dependence and marked improvement with methylphenidate treatment. Am J Psychiatry 1983; 140: 784-785. [ Links ]
68. Pandolfo P, Vendruscolo LF, Sordi R, Takahashi RN. Cannabinoid-induced conditioned place preference in the spontaneously hypertensive ratan animal model of attention deficit hyperactivity disorder. Psychopharmacology (Berl) 2009; 205: 319-326. [ Links ]
69. Rounsaville BJ, Anton SF, Carroll K, Budde D, Prusoff BA, Gawin F. Psychiatric diagnoses of treatment-seeking cocaine abusers. Arch Gen Psychiatry 1991; 48: 43-51. [ Links ]
70. Lambert NM, Hartsough CS. Prospective study of tobacco smoking and substance dependencies among samples of ADHD and non-ADHD participants. J Learn Disabil 1998; 31: 533-544. [ Links ]
71. Wilens TE, Adamson J, Sgambati S, Whitley J, Santry A, Monuteaux MC, et al. Do individuals with ADHD self-medicate with cigarettes and substances of abuse? Results from a controlled family study of ADHD. Am J Addict 2007; 16 (Suppl 1): 14-21. [ Links ]
72. Khantzian EJ. Self-regulation and self-medication factors in alcoholism and the addictions. Similarities and differences. Recent Dev Alcohol 1990; 8: 255-271. [ Links ]
73. Khantzian EJ. The self-medication hypothesis of substance use disorders: A reconsideration and recent applications. Harv Rev Psychiatry 1997; 4: 231-244. [ Links ]
74. Pontieri FE, Tanda G, Orzi F, Di Chiara G. Effects of nicotine on the nucleus accumbens and similarity to those of addictive drugs. Nature 1996; 382: 255-257. [ Links ]
75. Conners CK, Levin ED, Sparrow E, Hinton SC, Erhardt D, Meck WH et al. Nicotine and attention in adult attention deficit hyperactivity disorder (ADHD). Psychopharmacol Bull 1996; 32: 67-73. [ Links ]
76. Levin ED, Conners CK, Sparrow E, Hinton SC, Erhardt D, Meck WH, et al. Nicotine effects on adults with attention-deficit/hyperactivity disorder. Psychopharmacology (Berl) 1996; 123: 55-63. [ Links ]
77. Dougherty DD, Bonab AA, Spencer TJ, Rauch SL, Madras BK, Fischman AJ. Dopamine transporter density in patients with attention deficit hyperactivity disorder. Lancet 1999; 354: 2132-2133. [ Links ]
78. Krause KH, Dresel SH, Krause J, Kung HF, Tatsch K, Ackenheil M. Stimulant-like action of nicotine on striatal dopamine transporter in the brain of adults with attention deficit hyperactivity disorder. Int J Neuropsychopharmacol 2002; 5: 111-113. [ Links ]
79. Zuckerman M, Neeb M. Sensation seeking and psychopathology. Psychiatry Res 1979; 1: 255-264. [ Links ]
80. Zuckerman M. Sensation Seeking: beyond the optimal level of arousal. Hillsdale/NJ: Lawrence Erlbaum; 1979. [ Links ]
81. Hur YM, Bouchard TJ, Jr. The genetic correlation between impulsivity and sensation seeking traits. Behav Genet 1997; 27: 455-463. [ Links ]
82. Dresel S, Krause J, Krause KH, LaFougere C, Brinkbaumer K, Kung HF, et al. Attention deficit hyperactivity disorder: Binding of [99mTc]TRODAT-1 to the dopamine transporter before and after methylphenidate treatment. Eur J Nucl Med 2000; 27: 1518-1524. [ Links ]
83. Ernst M, Zametkin AJ, Matochik JA, Jons PH, Cohen RM. DOPA decarboxylase activity in attention deficit hyperactivity disorder adults. A [fluorine-18]fluorodopa positron emission tomographic study. J Neurosci 1998; 18: 5901-5907. [ Links ]
![]() Correspondence:
Correspondence:
Dr. Vanessa Prox-Vagedes, MD
Department of Psychiatry, Social Psychiatry and Psychotherapy
Hannover Medical School (MHH)
Carl-Neuberg-Straße 1
D-30625 Hannover, Germany
Tel.: 0049 / 511 532 3167
Fax: 0049 / 511 532 2415
Email: Prox-Vagedes.Vanessa@mh-hannover.de
Received: 30 May 2010
Revised: 14 February 2011
Accepted: 1 April 2011

