










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkThe European Journal of Psychiatry
Print version ISSN 0213-6163
Eur. J. Psychiat. vol.26 n.4 Zaragoza Dec. 2012
https://dx.doi.org/10.4321/S0213-61632012000400006
Cycloid psychoses: Leonhard´s descriptions revisited
Noortje W.A. van de Kerkhof*; Frank M.M.A. van der Heijden*; Marc K.F. Schneider*; Bruno Pfuhlmann**; Gerald Stöber**; Jos I.M. Egger*,***,****; Willem M.A. Verhoeven*,*****
* Vincent van Gogh Institute for Psychiatry, Centre of Excellence for Neuropsychiatry, Venray. The Netherlands
** University of Würzburg, Department of Psychiatry, Psychosomatics and Psychotherapy, Würzburg. Germany
*** Donders Institute for Brain, Cognition and Behaviour, Radboud University Nijmegen. The Netherlands
**** Behavioural Science Institute, Radboud University Nijmegen. The Netherlands
***** Erasmus University Medical Centre, Department of Psychiatry, Rotterdam. The Netherlands
ABSTRACT
Background and Objectives: Cycloid psychoses are characterized by polymorphic symptomatology with intraphasic bipolarity, a remitting and recurrent course and favourable prognosis. Perris and Brockington (P&B) described the first set of operational criteria that were partly incorporated in ICD-10. The present study investigates psychopathological profiles according to the P&B criteria and the original descriptions by Leonhard, both against the background of the criteria from the prevailing international classification systems.
Methods: Eighty patients with psychotic disorders were recruited and assessed with various psychometric instruments at baseline and after six weeks of antipsychotic treatment in order to investigate the presence of cycloid psychoses according to Leonhard (LCP) and the effect of treatment with antipsychotics. The overlap between LCP and DSM-IV Brief Psychotic Disorder (BPD), ICD Acute Polymorphic Psychotic Disorder (APP) and P&B criteria was calculated.
Results: Using P&B criteria and a symptom checklist adapted from the original descriptions by Leonhard, 14 and 12 cases of cycloid psychosis were identified respectively reflecting a prevalence of 15-18%. Small though significant concordance rates were found between LCP and both DSM-BPD and ICD-APP. Concordance between LCP and P&B criteria was also significant, but modest.
Conclusions: This study demonstrates that LCP can be identified in a substantial number of patients with psychotic disorders. Cycloid psychoses are not adequately covered in current classification systems and criteria. Since they are demonstrated to have a specific psychopathological profile, relapsing course and favourable prognosis, it is advocated to include these psychoses in daily differential diagnostic procedures.
Key words: Cycloid psychosis; Classification; Symptomatology; Leonhard; DSM-IV; ICD-10.
Introduction
As an independent group, the term "cycloid psychoses" was first coined by Kleist in 19261. Psychoses with atypical symptoms had been described from the turn of the nineteenth century and were termed e.g., "bouffées délirantes des dégenerées"2, "Degenerationspsychose"3, acute schizoaffective psychosis4, "degeneratiepsychose"5 and atypical psychosis6. About two decades ago, the psychopathological concepts about this type of psychoses were reviewed in detail by Tappe7.
In general, cycloid psychoses present with a (sub)acute onset and a polymorphic and shifting symptomatology comprising symptoms from both the schizophrenic and affective spectrum. Depending on the subtype, most typical symptoms are rapid mood swings, severe anxiety and/or ecstasy, confusional states and psychomotor disturbances8-11. In the fifties, based on the detailed longitudinal analysis of symptom profiles, Leonhard delineated three subtypes: anxiety-happiness psychosis, confusion psychosis and motility psychosis12. Later, Pfuhlmann and coworkers found high interrater reliability (Cohen's kappa: 0.82-0.89) of Leonhard's classification system13.
As to prognosis, cycloid psychoses show a remitting and recurrent course with a favou-rable outcome14-16. The only study on the pharmacological treatment of cycloid psychoses has demonstrated beneficial effects of lithium17. More recently, some evidence has been obtained that, in the acute phase, atypical antipsychotics may be useful18.
Although in 1952 the first edition of the DSM comprised a psychotic disorder with atypical symptoms resembling some features of the cycloid psychosis (termed schizophrenic reaction, acute undifferentiated type), later versions did not cover this diagnostic category. In fact, Kraepelin's dichotomy increasingly dominated the categorical structure in the consecutive editions of the DSM so that in DSM-IV19, only Brief Psychotic Disorder (BPD) and Schizophreniform Disorder with specifier "With Good Prognostic Features" partially cover the cycloid concept. This development and the increase of the clinical diagnosis of schizoaffective disorders resulted in a gradual loss of scientific and clinical interest for the cycloid psychoses. Recently, in their scholarly review, Jäger and coworkers stipulated the problematic reliability and validity of schizoaffective disorder and hinted at a fundamental reconsideration of the current diagnostic concepts of psychosis20. Similar suggestions were made by the research group of García-Andrade21. Therefore, the cycloid psychosis postulate needs to be revisited, particularly given its relevance for clinical practice.
The first set of operational criteria for cycloid psychoses was formulated by Perris and Brockington22 and subsequently incorporated in the "Diagnostic Criteria for Functional Psychoses" of the World Psychiatric Association23. Starting with the ICD-1024, the category acute polymorphic psychotic disorder without/with symptoms of schizophrenia (APP) is included that was derived from the Perris and Brockington (P&B) criteria. This category comprises, apart from cycloid psychosis, also the psychotic disorder bouffée délirante, used in France as a separate diagnostic category.
Clinical studies in patients with Leonhard's cycloid psychoses (LCP), using brain imaging25 and event related potentials26,27, have demonstrated that, in addition to variability in symptomatology, course, and prognosis, this class of psychoses is etiologically distinct from schizophrenia and bipolar affective disorders28,29. In rare cases of cycloid psychosis, disturbances in amino acid metabolism were observed30,31. Hereditary factors have been demonstrated to play a minor role32,33, whereas environmental factors like maternal first-trimester gestational infection and obstetrical complications, seem to be of etiological importance34,35. Cycloid psychoses predominate in postpartum psychotic disorders36,37.
The present study aims at delineating cycloid psychoses according to Leonhard's original descriptions and analyzes the diagnostic overlap with P&B as well as with ICD-10 and DSM-IV criteria.
Methods
Patient recruitment
All patients were recruited at the Vincent van Gogh Institute for Psychiatry, a large psychiatric teaching hospital in the southern part of The Netherlands with a catchment area of ~510.000 inhabitants. The recruitment period comprised 2.5 years (March 2008-September 2010).
Included were adult patients of both sexes (age range: 18-65 yrs) admitted for psychotic symptomatology that warranted treatment with psychotropics. Patients were included before the start or in the first week of treatment with psychotropics. In all cases, psychopharmacological treatment was performed according to the hospital standards by the responsible ward psychiatrist. Excluded were patients with proven genetic syndromes or intellectual disability. For this reason, a genetic work-up was performed by a registered clinical geneticist. Also excluded were patients with relevant somatic or neurologic diseases and females with postpartum psychopathology. All patients gave written informed consent following the Dutch medical ethical guidelines (CCMO registration number NL20469.097.07).
During the study period, a total of 194 patients were admitted for evaluation and treatment of psychotic symptoms of whom 100 were judged to be eligible for inclusion. Twenty patients refused to participate yielding a study group of 80 patients of whom 63 were available for follow-up assessment after at least 6 weeks (i.e., 63% of the initial selected group).
Diagnostic procedures and scoring instruments
Baseline diagnostic instruments comprised Comprehensive Assessment of Symptoms and History (CASH)38, Positive and Negative Syndrome Scale (PANSS)39, and Clinical Global Impression scales for Severity and Improvement (CGI-S/CGI-I)40. The CASH was specifically developed for research in the schizophrenia and affective spectrum conditions and is not uniquely connected to a classification system. PANSS and CGI were re-assessed at week 6. These assessments were performed by a well trained PhD-resident in psychiatry (NvdK).
Subsequently, classification was perfor-med according to DSM-IV19 and ICD-1024 by NvdK and FvdH. Independently, the criteria for cycloid psychoses as advanced by Perris and Brockington23 were applied to all subjects by a psychiatrist specifically trained in the diagnosis of cycloid psychosis (MS). In addition, using the symptom checklist of Leonhard12,41 (Table 1), an internationally recognized psychiatrist (GS) delineated patients with LCP. Accordingly, a division into the three subtypes of cycloid psychosis was performed.

Analogous to a so called LEAD conference42, in a final meeting with all investigators chaired by an independent experienced psychiatrist (WV), all available classificatory data were discussed to analyse the differential application of the various sets of criteria.
Statistics
For all statistic procedures, SPSS 14.0 software was used. Group differences were tested using the Student's t-test for continuous variables and Chi-square test for nominal variables. Cohen's kappa was used to test the concordance between the different categorical diagnostic groups. Significance was tested against p < 0.05.
Results
Total patient sample and symptomatic reduction after 6 weeks
The total group comprised 53 males and 27 females (mean age ± SD: 35 ± 11.5). Mean age at first episode and mean duration of psychotic disease were 27.4 ± 10.7 and 7.6 ± 7.9 years respectively. According to DSM-IV, 48 patients met the criteria for Schizophrenia. The remaining 32 patients fulfilled diagnostic criteria for Brief Psychotic Disorder: n = 10, Psychotic Disorder NOS: n = 7; Bipolar Disorder: n = 7; Schizoaffective Disorder: n = 5; Delusional Disorder: n = 2; and Schizotypal Disorder: n = 1.
Patients were treated with classical/first generation (n = 27) and atypical/second generation (n = 61) antipsychotics, either as monotherapy (n = 72) or in combination (n = 8). After six weeks of treatment, scores on the PANSS total, positive, negative and global scales decreased from 86 to 69 (20%), 23 to 17 (26%), 20 to 17 (15%) and 43 to 35 (19%) respectively. The CGI-S improved from 4.5 to 3.4 (23%). All comparisons were statistically significant (p < 0.001).
Diagnosis of cycloid psychoses according to P&B criteria and Leonhard
Concerning cycloid psychosis according to P&B, 14 patients (18%) met the criteria. According to Leonhard's descriptions, in 12 patients a cycloid psychosis was present reflecting a prevalence of 15%. Leonhard's cycloid psychoses could be further specified as anxiety-happiness psychosis (n = 5), confusion psychosis (n = 3), and motility psychosis (n = 4). Brief case vignettes are depicted in Table 2.

Of the 14 patients with P&B cycloid psychosis, 9 also accorded with Leonhard's descriptions (Table 2: no. 1-4, 6-9, and 11).
In Table 3, the main characteristics of the non-cycloid (n = 68) and LCP (n = 12) patient groups with their corresponding DSM-IV, ICD-10 and P&B diagnoses are presented. As can be inferred, the LCP subgroup has a higher age at onset of both psychosis and general psychiatric symptoms. LCP as well as non-CP groups show diagnostic heterogeneity, albeit that a diagnosis of schizophrenia, according to ICD and DSM, is exclusively made in the non-CP group. In the LCP group, diagnoses of DSM-IV Brief Psychotic Disorder or ICD-10 Acute and Transient Psychotic Disorder are represented more often.

With respect to severity of symptomatology as assessed with the PANSS, total scores at baseline did not reveal differences between the two groups. After 6 weeks of treatment with antipsychotics in a naturalistic setting, however, the symptomatic decrease was more pronounced in the cycloid group (p < 0.01).
Psychopathology
Detailed analysis of the individual symptomatology of the LCP patients (n = 12) and those who met the P&B criteria (n = 14), revealed that the seven symptoms "ecstatic elation", "altruistic ideas of happiness", "rapidly changing anxiety and euphoria", "pressure of speech with incoherence of thematic choice", "confused stupor", "psychomotor excitement with increased expressive and reactive movements" and "stupor with stiff posture" (Table 1, symptom checklist items 4-6, 10, 15, 17 and 22) are most prevalent in both or either group of patients, indicating that bipolarity of mood, thought and locomotion, frequently occurring also intraphasic, are key symptoms of cycloid psychosis. Moreover, these key symptoms are virtually identical to those from the extreme poles as originally described by Leonhard.
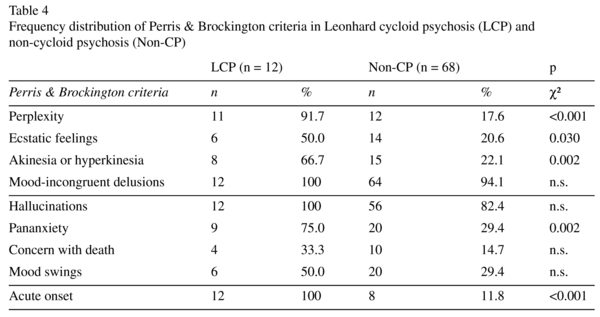
Table 4 illustrates the symptom profile of the 12 patients with LCP as compared to the group of non-cycloid psychosis (n = 68) by applying the P&B criteria. Whereas delusions and hallucinations are present in most of the patients in both groups, the atypical symptoms (perplexity, ecstatic feelings, mo-tility disorders and pananxiety) are overrepresented in the LCP subgroup.
Cycloid psychosis: representation in ICD/DSM and concordance rates
Concordance rates were calculated for LCP (n = 12) and the most frequent DSM-IV and ICD-10 diagnoses in this group (see: Table 3). Between LCP on the one hand and ICD-APP and DSM-BPD on the other hand a concordance rate of 0.58 and 0.35 (both p < 0.001) was present respectively (Figure 1a,b). A concordance rate of 0.63 (p < 0.001) was calculated between LCP diagnosis according to Leonhard's symptom checklist and P&B criteria whereas a rate of 0.38 (p < 0.001) was found between LCP and ICD schizoaffective disorder (SAD) (Figure 1c,d). The concordance between LCP and DSM-SAD did not reach statistical significance.

Discussion
In this observational study with a group of patients admitted for psychotic disorders, the presence of cycloid psychoses according to both Leonhard's descriptions and the criteria as established by Perris and Brockington, was investigated. A prevalence rate of 15% was found for Leonhard's cycloid psychoses. It appeared that cycloid psychosis can also be diagnosed according to the P&B criteria, whereas application of Leonhard's descriptions additionally provides differentiation in the three subtypes.
The highest concordance was calculated between LCP and P&B, whereas lower concordance rates emerged between LCP and the different ICD-10 (APP and SAD) and DSM-IV (BPD) categories (Figure 1a-d).
With respect to the prevalence of cycloid psychosis, the here observed frequency of 15% is in accordance with that reported by other investigators (8-24%)14,43-46. The prevalence from this study may, however, be biased negatively since female patients with postpartum psychopathology were a priori excluded and the sample size was limited due to the strict inclusion criteria as defined by the Dutch ethical rules for genetic work-up and for patients admitted under a legal act. Still, the overrepresentation of female patients in our cycloid group is in line with the results from other studies11,14,47.
Since the majority of the patients who were diagnosed as LCP were classified as ICD-10 APP or DSM-IV BPD, the concordance rates between these categories are most relevant (Figure 1a,b). Albeit that the observed values are higher than those reported by Pillmann and coworkers47 with ICD-10 Acute and Transient Psychotic Disorders (including APP) of 0.36 and by Van der Heijden and coworkers46 with 0.24 for BPD and 0.31 for APP, it has to be underlined that in the latter studies, patients were classified according to P&B criteria only. This suggests that the criteria for DSM-BPD and ICD-APP do neither cover sufficiently the descriptions by Leonhard nor the P&B criteria and that particularly Leonhard's symptom checklist is most promising for clinical practice. It has to be stressed, however, that this study is the first to systematically investigate this checklist on its relation to classification systems and thus needs further scientific evaluation.
The observed discrepancies in overlap between LCP and both ICD-APP and DSM-BPD may be explained by the duration criterion. In DSM-IV as well as ICD-10, a maximum duration of 1 to 3 months is required which excludes a priori the cycloid psychoses that are characterized by highly variable duration and frequently relapsing course18,35,48-51.
As can be inferred from Figure 1c, the concordance rate between LCP and P&B is also rather moderate which may be due to the onset and age criteria, in that the onset criterion in P&B comprises a time interval of hours to days, while in LCP this is not quantified. Moreover, in P&B the criterion age is restricted to the range 15-50 years, while according to the original monograph, LCP does not comprise any age limitation. That three LCP cases are discordant with P&B cycloid psychosis, is explained by the age criterion (> 50 years old at first presentation; n = 2) or the required number of symptoms (≥ 4; n = 1). With respect to the overlap between LCP and SAD, it has to be stressed that this finding is rather irrelevant since the SAD as included in the ICD-10 and DSM-IV cannot be compared with the acute schizoaffective psychosis as originally described by Kasanin4 and is not clearly demarcated from schizophrenia and affective disorders20.
As demonstrated in the present study, the three subtypes of cycloid psychosis can clearly be discriminated from other psychotic disorders by their pronounced symptomatological presentation and intraphasic bipolarity (Table 1). Key features of their core syndromes include perplexity, pananxiety, motor disturbances, mood swings and transient hallucinatory experiences of any kind.
Interestingly, in the cycloid psychosis group a higher symptom reduction was found after 6 weeks on antipsychotics from various classes. Although not the main target of the present investigation, the pharmacological maintenance treatment of cycloid psychoses is suggested to be primarily with mood stabilizers17,52 whereas in the acute phase atypical antipsychotics may be beneficial18. Generally, these psychoses have a good prognosis15,35,48,53 and their diagnostic stability is high54,55.
In conclusion, the results demonstrate that the concept of cycloid psychosis is still clinically useful and valid. It would be therefore wise to include a separate group of nonaffective acute psychoses in the future editions of current international classification systems. Such a proposal was recently also formulated by Nugent and coworkers56. Given the rather high prevalence of this kind of psychosis, further clinical studies with differential assessment methods such as Leonhard's symptom checklist are warranted and should particularly focus on treatment strategies and long term outcome.
Acknowledgment
The authors are indebted to the patients for their willingness to participate in the study and to the medical and nursing staff of the wards for their cooperation in recruiting the patients. Statistical analyses were performed by No E.S. Sijben, Msc, PhD from ABC/OPES in Velp, The Netherlands. Special thanks to Prof. Dr. Jos I.M. Egger, clinical neuropsychologist for his assistance in preparing the final version of the manuscript.
References
1. Kleist K. Über zykloide Degenerationspsychosen, besonders Verwirrtheits- und Motilitätspsychosen. Zentralbl Ges Neurol Psychiat 1926; 44: 655-657. [ Links ]
2. Magnan V. Leçons cliniques sur les maladies mentales. Paris: Progrès Médical Alcan; 1897. [ Links ]
3. Bonhoeffer K. Klinischer beitrag zur lehre von den degenerationspsychosen. Halle: Marhold; 1907. [ Links ]
4. Kasanin J. The acute schizoaffective psychoses. Am J Psychiatry 1933; 13: 97-126. [ Links ]
5. Van der Spek PAF. Over de klinische waarde van het begrip degeneratiepsychose. Thesis, Universiteit van Amsterdam; 1940. [ Links ]
6. Mitsuda H. The concept of "atypical psychoses" from the aspect of clinical genetics. Acta Psychiatr Scand 1965; 41: 372-377. [ Links ]
7. Tappe K. Synonymy of phasic "atypical" psychoses - cycloid psychoses versus other classifications. In: Beckmann H, Neumärker KJ, editors. Endogenous psychoses. Berlin: Ullstein Mosby; 1995. p. 90-111. [ Links ]
8. Leonhard K. Cycloid psychoses: Endogenous psychoses which are neither schizophrenic nor manic-depressive. J Ment Sci 1961; 107: 633-648. [ Links ]
9. Leonhard K. Classification of endogenous psychoses and their differentiated etiology. (2nd ed.). Wien: Springer Verlag; 1999. [ Links ]
10. Perris C. A study of cycloid psychoses. Acta Psychiatr Scand 1974; 253: S1-77. [ Links ]
11. Perris,C. The concept of cycloid psychotic disorder. Psychiatr Dev 1988; 6: 37-56. [ Links ]
12. Leonhard K. Aufteilung der endogenen Psychosen. Berlin: Akademie; 1957. [ Links ]
13. Pfuhlmann B, Franzek E., Stöber G., Cetkovich-Bakmas M, Beckmann H. On interrater reliability for Leonhard's classification of endogenous psychoses. Psychopathology 1997; 30: 100-105. [ Links ]
14. Cutting JC, Clare AW, Mann AH. Cycloid psychosis: An investigation of the diagnostic concept. Psychol Med 1978; 8: 637-648. [ Links ]
15. Jabs BE, Krause U, Althaus G, Bartsch AJ, Stöber G, Pfuhlmann B. Differences in quality of life and course of illness between cycloid and schizophrenic psychoses - a comparative study. World J Biol Psychiatry 2004; 5: 136-142. [ Links ]
16. Menuck M, Legault S, Schmidt P, Remington G. The nosological status of the remitting atypical psychoses. Compr Psychiatry 1989; 30: 53-73. [ Links ]
17. Perris C. Morbidity suppressive effect of lithium carbonate in cycloid psychosis. Arch Gen Psychiatry 1978; 35: 328-331. [ Links ]
18. Jabs BE, Pfuhlmann B, Bartsch AJ, Cetkovich-Bakmas M, Stöber G. Cycloid psychoses - from clinical concepts to biological foundations. J Neural Transm 2002; 109: 907-919. [ Links ]
19. American Psychiatric Association. Diagnostic and statistic manual of mental disorders. (4th ed.). Washington: American Psychiatric Association; 1994. [ Links ]
20. Jäger M., Haack S, Becker T, Frasch K. Schizoaffective disorder-an ongoing challenge for psychiatric nosology. Eur Psychiatry 2011; 26: 159-165. [ Links ]
21. García-Andrade RF, Díaz-Marsá M, Carrasco JL, López-Micó C, Saiz-Gonzalez D, Aurecoecha JF, et al. Diagnostic features of the cycloid psychoses in a first psychotic episode sample. J Affect Disord 2011; 130: 239-244. [ Links ]
22. Perris C, Brockington IF. Cycloid psychoses and their relation to the major psychoses. In: Perris C, Struwe D, Jansson B, editors. Biological Psychiatry. Amsterdam: Elsevier; 1981. p. 447-450. [ Links ]
23. Berner P, Gabriel E, Katschnig H, Kieffer W, Koehler K, Lenz G, et al. Diagnostic criteria for functional psychoses. Cambridge: University Press; 1992. [ Links ]
24. World Health Organization. The ICD-10 classification of mental and behavioural disorders. Clinical descriptions and diagnostic guidelines. Geneva: World Health Organization; 1992. [ Links ]
25. Höffler J, Bräunig P, Krüger S, Ludvik M. Morphology according to cranial computed tomography of first-episode cycloid psychosis and its long-term-course: Differences compared to schizophrenia. Acta Psychiatr Scand 1997; 96: 184-187. [ Links ]
26. Strik WK, Fallgatter AJ, Stoeber G, Franzek E. Specific P300 features in patients with cycloid psychosis. Acta Psychiatr Scand 1997; 95: 67-72. [ Links ]
27. Strik WK, Ruchsow M, Abele S, Fallgatter AJ, Mueller TJ. Distinct neurophysiological mechanisms for manic and cycloid psychoses: Evidence from a P300 study on manic patients. Acta Psychiatr Scand 1998; 98: 459-466. [ Links ]
28. Beckmann H, Franzek E. Cycloid psychoses and their differentiation from affective and schizophrenic psychoses. In: Henn F, Sartorius N, Helmchen H, Lauter H, editors. Contemporary Psychiatry, vol. 3. Heidelberg: Springer; 2001. p. 387-398. [ Links ]
29. Pfuhlmann B, Jabs B, Althaus G, Schmidtke A, Bartsch A, Stöber G, et al. Cycloid psychoses are not part of a bipolar affective spectrum. Results of a controlled family study. J Affect Disord 2004; 83: 11-19. [ Links ]
30. Pepplinkhuizen L, Bruinvels J, Blom W, Moleman P. Schizophrenia-like psychosis caused by a metabolic disorder. Lancet 1980; 454-456. [ Links ]
31. Pepplinkhuizen L, Van der Heijden FMMA, Tuinier S, Verhoeven WMA, Fekkes D. The acute transient polymorphic psychosis: A biochemical subtype of the cycloid psychosis. Acta Neuropsychiatr 2003; 15: 38-43. [ Links ]
32. Franzek E, Beckmann H. Different genetic background of schizophrenia spectrum psychosis: A twin study. Am J Psychiatry 1998; 155: 76-83. [ Links ]
33. Leonhard K. Aufteilung der endogenen Psychosen und ihre differenzierte Ätiologie (8th ed.). Stuttgart: Georg Thieme Verlag; 2003. [ Links ]
34. Stöber G, Kocher I, Franzek E, Beckmann H. First-trimester maternal gestational infection and cycloid psychosis. Acta Psychiatr Scand 1997; 96: 319-324. [ Links ]
35. Maj M. Cycloid psychotic disorder: Validation of the concept by means of a follow-up and a family study. Psychopathology 1990; 23: 196-204. [ Links ]
36. Lanczik M, Fritze J, Beckmann H. Puerperal and cycloid psychoses: Results of a retrospective study. Psychopathology 1990; 23: 220-227. [ Links ]
37. Pfuhlmann B, Stöber G, Franzek E, Beckmann H. Cycloid psychoses predominate in severe postpartum psychiatric disorders. J Affect Disord 1998; 50: 125-134. [ Links ]
38. Andreasen NC, Flaum MC, Arndt S. The comprehensive assessment of symptoms and history (CASH): An instrument for assessing diagnosis and psychopathology. Arch Gen Psychiatry 1992; 49: 615-623. [ Links ]
39. Kay SR, Fiszbein A, Opfer LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull 1987; 13: 261-276. [ Links ]
40. Guy W. ECDEU assessment manual for psychopharmacology. Revised. Bethesda: National Institute of Mental Health; 1976. [ Links ]
41. Leonhard K. Differenzierte Diagnostik der endogenen Psychosen unter Anlehnung an einen Symptomenkatalog. Psychiatr Neurol Med Psychol 1990; 42: 136-145. [ Links ]
42. Skodol AE, Rosnick L, Kellmann D, Oldham JM, Hyler S. Development of a procedure for validating structured assessment of axis II. In: Oldham JM, editor. Personality disorders: New perspectives on diagnostic validity. Washington: American Psychiatric Press; 1991. p. 43-70. [ Links ]
43. Lindvall M, Axelsson R, Öhman R. Incidence of cycloid psychosis: A clinical study of first-admission psychotic patients. Eur Arch Psychiatry Clin Neurosci 1993; 242: 197-202. [ Links ]
44. Modestin J, Rausch A, Sonderegger P, Bachmann KM, Erni T. Clinical study on cycloid psychosis. Eur J Psychiat 2002; 16: 95-101. [ Links ]
45. Peralta V, Cuesta MJ. Cycloid psychosis. Int Rev Psychiatry 2005; 17: 53-62. [ Links ]
46. Van der Heijden FMMA, Tuinier S, Kahn RS, Verhoeven WMA. Nonschizophrenic psychotic disorders: The case of cycloid psychoses. Psychopathology 2004; 37: 161-167. [ Links ]
47. Pillman F, Haring A, Balzuweit S, Blöink R, Marneros A. Concordance of acute and transient psychoses and cycloid psychoses. Psychopathology 2001; 34: 305-311. [ Links ]
48. Brockington IF, Perris C, Kendell RE, Hillier VE, Wainwright S. The course and outcome of cycloid psychosis. Psychol Med 1982; 12: 97-105. [ Links ]
49. Marneros A, Pillmann F, Haring A, Balzuweit S. Die akuten vorübergehenden psychotischen Störungen. Fortschr Neurol Psychiatr 2000; 68: S22-25. [ Links ]
50. Peralta V, Cuesta MJ. Cycloid psychosis: a clinical and nosological study. Psychol Med 2003; 33: 443-453. [ Links ]
51. Salvatore P, Bhuvaneswar C, Ebert D, Maggini C, Baldessarini RJ. Cycloid psychoses revisited: Case reports, literature review, and commentary. Harv Rev Psychiatry 2008; 16: 167-180. [ Links ]
52. Perris C. Cycloid psychotic disorders ("marginal psychoses"). In: Seva A, editor. The European handbook of psychiatry and mental health. Zaragoza: Prensas Universitarias de Zaragoza; 1991. p. 1000-1009. [ Links ]
53. Beckmann H, Fritze J, Lanczik M. Prognostic validity of the cycloid psychoses: A prospective follow-up study. Psychopathology 1990; 23: 205-211. [ Links ]
54. Pethö B, Tolna J, Tusnády G, Farkas M, Vizkeleti G, Vargha A, et al. The predictive validity of the Leonhardean classification of endogenous psychoses. Eur Arch Psychiatry Clin Neurosci 2008; 258: 324-334. [ Links ]
55. Von Trostorff S, Leonhard K. Catamnesis of endogenous psychoses according to the differential diagnostic method of Karl Leonhard. Psychopathology 1990; 23: 259-262. [ Links ]
56. Nugent KL, Paksarian D, Mojtabai R. Nonaffective acute psychoses: Uncertainties on the way to DSM-V and ICD-11. Curr Psychiatry Rep 2011; 13: 203-210. [ Links ]
![]() Correspondence:
Correspondence:
Mrs. N.W.A. van de Kerkhof, M.D.
Vincent van Gogh Institute for Psychiatry
Stationsweg 46
5803 AC Venray
The Netherlands
Phone: +31478527339
Fax: +31478527111
E-mail: nvandekerkhof@vvgi.nl
noortjevandekerkhof@gmail.com
Received: 13 March 2012
Revised: 11 June 2012
Accepted: 16 July 2012

