










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkThe European Journal of Psychiatry
Print version ISSN 0213-6163
Eur. J. Psychiat. vol.27 n.2 Zaragoza Apr./Jun. 2013
https://dx.doi.org/10.4321/S0213-61632013000200006
Familiarity with and Attitudes to Tourette's Syndrome in Healthcare Students: A Pilot Comparison with Epilepsy
Cara Katona MB BS
University Hospital of North Staffordshire, Stoke on Trent. United Kingdom
ABSTRACT
Background and Objectives: Tourette's Syndrome (TS) is a common developmental neuropsychiatric disorder; people with TS are vulnerable to stigmatization. Public attitudes to TS have seldom been studied. This study examines knowledge of and attitudes to TS and to epilepsy in healthcare students, in an attempt to explore and compare the stigma which might be attached to the two conditions.
Methods: Questionnaire survey of healthcare students at one UK medical school.
Results: 94 students responded. Though more students knew someone with epilepsy than someone with TS (57% vs 15%; p<0.0001), they were more likely to know a public figure with TS (37% vs 12%; p<0.0001). Among medical students, a higher proportion has seen someone showing evidence of TS (63%) than had seen anyone having a fit (43%; p<0.05). As many as 26% of medical students would object to having a son or daughter of theirs marry a person with TS and 19% of people would object to the marriage of one of their children to a person with epilepsy.
Conclusions: The majority of healthcare students had some familiarity with and did not have negative attitudes towards people with TS. However there is still some degree of stigmatization towards both conditions. There remains scope for education in this area as well as for extending such survey research on TS to the general population. Study limitations include the small sample size, and the fact that healthcare students are unrepresentative of broader public opinion.
Key words: Tourette's Syndrome; Epilepsy; Attitudes; Healthcare students.
Introduction
Tourette's Syndrome (TS) is "a developmen-tal neuropsychiatric disorder defined by the presence of otherwise unexplained multiple motor tics and at least one vocal/phonic tic for the duration of one year and with onset before age 21 years"1. Reported prevalence rates vary widely but recent studies suggest a figure of about 1% in young people aged 5-18 (ibid). It is classified as a syndrome because its aetiology is unknown, though genetic factors, neurotransmitter abnormalities and infectious agents have been implicated2.
Although the general public have become more aware of TS (in part because of media and publicity campaigns) "the syndrome is still perceived as rendering life difficult for people who have it"3. The authors of this analysis of the TS experience from an anthropological perspective conclude that people with TS "are often stigmatised by their behavior", and also by distorted interpretations of that behaviour by those around them. A further important factor recently has been the media portrayal of TS: "representations of the 'cursing disease' have become common in the mainstream media and entertainment industries. Celebrities casually call themselves "Touretters" when they misspeak or are held accountable for excessive cursing" (ibid).
In a study of the attitudes of high school pupils to TS, Brook and Boaz4 point out that the potential for stigmatization of TS is enhanced by comorbid conditions such as obsessive compulsive disorder (OCD) and attention deficit hyperactivity disorder (ADHD), each of which is present in a high proportion (perhaps two thirds) of people with TS. Their study (which used an unpublished questionnaire) concluded that greater tolerance towards TS was determined by increasing age, better school grades and family experience of mental health problems.
A search of the Medline database using the terms "stigma" and "Tourette" did not identify any relevant studies other than those cited above. In particular there appear to have been no studies of the attitudes of the adult public to TS and no studies comparing attitudes to TS with those to other neurological or psychiatric conditions.
Epilepsy is in several respects a comparable condition to TS, but it is one in which public attitudes have been studied extensively. The prevalence of epilepsy is about 0.7%5 though unlike TS its onset is less consistently in childhood. Epilepsy, like TS, is a stigmatising condition; the World Health Organization highlights the widespread legislation in place until quite recently in many countries limiting rights to marriage, healthcare and even access to public places (www.who.int/mediacentre/factsheets/fs999/en/index.html). Impaired quality of life in people with epilepsy (PWE) results both from such legislative limitations and from stigmatizing public attitudes. Caveness and Gallup6 found that public attitudes to PWE had become substantially less negative between the 1940s and 1970s. A more recent study in Austria by Spat et al.7 summarises the many such surveys of public attitudes to PWE across the world. In general negative attitudes are associated with being male, of low socio-economic status and having low educational attainment.
The main aim of this pilot study is to compare knowledge of and attitudes to people with TS and PWE in healthcare students within a UK university (St George's University of London), and to examine the effect of gender on such attitudes and on the degree with which people with the two conditions are stigmatized. A further focus is on whether a particular media event (the participation in, and victory of, a young man with TS in the 2006 Big Brother reality television show - http://en.wikipedia.org/wiki/Pete_Bennett) has increased public familiarity with TS. In the pilot study that is reported in this paper, a sample of healthcare students at a single university is surveyed. A further aim is to establish whether the TS-adapted survey instrument provides useful information on knowledge of and attitudes towards TS, with a view to carrying out studies in broader population samples.
Methods
Design of Survey Instrument
The survey instrument (see Appendix) was based on a questionnaire developed by the American Institute of Public Opinion to "gain some concept of attitudes throughout the United States towards epilepsy as it related to the intellectual, social and economic spheres of our society"6. Each question from that survey was used both in its original form and in an adapted form with TS substituted for epilepsy. An extra question was added (again in versions both for Epilepsy and TS) asking whether the respondent could name a public figure with the condition.

Administration of Survey
The survey questionnaire was uploaded onto Survey Monkey (http://www.surveymonkey.com) and the survey specific URL was published in the weekly St George's student newsletter in February 2009. Students were also encouraged to complete the survey through individual emails that included the URL.
Analysis
Summary statistics were generated by the Survey Monkey software (http://www.surveymonkey.com). Comparisons between TS and epilepsy responses were compared using the chi-square test or Fisher's exact test, using Graphpad software (http://www.graphpad.com/quickcalcs/contingency1.cfm).
Results
The sample
There were a total of 2395 eligible students at St George's University of London (58% of them female). Of these 1415 were medical students, among whom 56% were female.
A total of 94 questionnaires were completed. The demographic characteristics of the students who filled in questionnaires are summarised in Table 1.

About two thirds of the participants were female; the age distribution was skewed, with a range between 19 and 37, but with both mode and median at age 22. All but 9 of the participants were studying medicine with the largest single group studying on the 5 year medical programme. Nearly half the respondents were in the third year of their course.
Questionnaire responses
Responses to each of the 8 questions for TS and for Epilepsy are summarised in table 2. Table 3 shows the responses obtained from the subsample of 5-year course medical students.

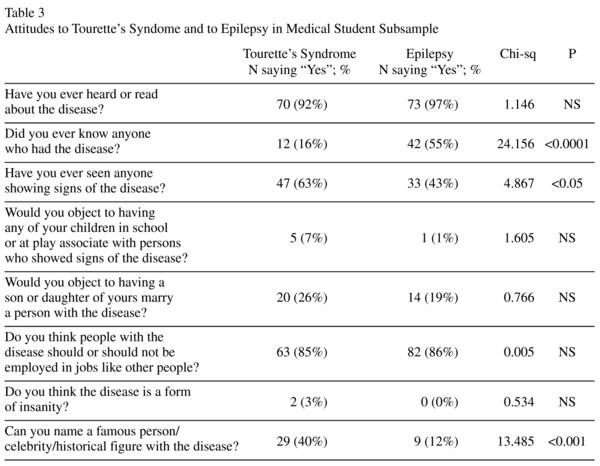
As can be seen in Table 2, a much high proportion of respondents knew someone personally with epilepsy than someone with TS (57% vs 15%; p<0.0001). In contrast, a higher proportion knew of a famous person with TS than with epilepsy (37% vs 12%; p<0.0001). In 24 of respondents able to identify someone with TS, it was Pete Bennett, the winner of Big Brother 2006. All but one of the other positive responses to this question identified the footballer Tim Howard. The same differences were evident in the 5-year medical programme students (Table 3); in this subsample it was also evident that a higher proportion has seen someone showing evidence of TS (63%) than had seen anyone having a fit (43%; p<0.05). 26% of medical students would object to having a son or daughter of theirs marry a person with TS and 19% of people would object to the marriage of one of their children to a person with epilepsy.
When the responses were broken down by gender, the only significant differences related to epilepsy. Female students were more likely to know someone with epilepsy (43/65 vs 11/28; Chi-sq = 4.751, p<0.05) and male students were more likely to think that people with epilepsy should not be in normal jobs (7/29 vs 5/65; Fisher's exact test p<0.05). There was a non-significant trend for female students to be more likely to have seen someone showing signs of TS (43/64 vs 13/29; p<0.1).
There were no significant differences in responses to the other TS-related questions between people who had heard of a famous person with TS and those who had not.
68/94 respondents answered an open text question about causes of TS. This was a significantly lower proportion than answered the same question about epilepsy (82/94 positive responses; chi-sq = 5.574; p<0.05). The most frequent answers relating to causes of TS were unknown -15; genetic - 12; neuro-anatomic - 10; and neuro-chemical - 6.
Discussion
Overall, students completing this survey had much more positive attitudes to epilepsy than the general population samples reported by Caveness and Gallup6 and by Spatt et al.7 This is likely to reflect their commitment to medicine and other healthcare professions as well as to continuing recent improvements in public attitudes to chronic illness.
The results indicate relatively modest differences in knowledge of and attitudes towards TS and to epilepsy in healthcare students. The key differences were that students were less likely to know someone with TS but more likely to be able to name a famous person with the condition. Together with the finding that two thirds of those identify someone with TS invoking Pete Bennett, these results strongly support the hypothesis that the publicity that Pete Bennett generated has increased familiarity with TS, at least within the young student public. The absence of clear differences in attitudes to TS between those who could and could not identify someone with the condition makes it impossible to conclude that the "Pete Bennett effect" has had a positive effect on attitudes, but may of course simply reflect small numbers and lack of statistical power.
It is worrying that, even among healthcare students, as many as 22% would object to their children marrying someone with TS and 5% would not even wish their child to play with someone with TS. In both cases the proportion objecting in these ways to TS was higher (though not significantly so) than for epilepsy, suggesting there remains a need for substantial positive change in public attitudes to TS in order to achieve "catch-up" with improving public attitudes to PWE. There are a number of possible explanations for the stigma that exists towards TS. Perhaps the most obvious reason for the stigma is that TS is a condition which many people have not been taught about. This ignorance breeds fear; people are scared of what they do not understand. As a result, tics, rather than being regarded as a symptom of a condition, may be considered as unpredictable, threatening and even frightening behaviour. This stigmatization is exaggerated further by the fact that TS may wrongly be associated with mental health problems such as schizophrenia - itself a widely misunderstood and thus stigmatized condition. One limitation of the present study is that we were unable (because of limitations in data that could be extracted from Survey Monkey) to examine the putative association between knowledge of TS or epilepsy on the one hand, and attitudes to each condition on the other.
It must also be borne in mind that TS and epilepsy are not wholly equivalent. People with TS have been reported to have greater subjective impairment in quality of life than PWE8 as well as having distinct patterns of obsessive-compulsive psychopathology than comparison subjects with temporal lobe epilepsy9.
These results do not indicate large differences in attitude between female and male students, but do show (in keeping with the findings reported and summarised by Spatt et al. 2005) that women are more likely to be knowledgeable about epilepsy.
The present study has important limitations and should be regarded as an exploratory or pilot investigation. The sample size is small and the response rate very low. Although the intention was to make the survey representative of healthcare students, medical students and third year students (i.e. those in the same year and subject as the author) are over-represented. The response rate was also higher in female students than in males. The sample studied may also be self-selected in terms of having relatively positive attitudes. Unfortunately it was not possible to send out a mass email to all students as originally intended. It is hoped to be able to do so, and thereby to collect a larger and more representative sample. This would make it possible to compare responses by year of study and by subject studied. The study is also limited in that its findings cannot be extrapolated to the general population. The sample studied was however chosen not only because recruitment was relatively straightforward, but also because health care students are the people who in the future will be caring for epilepsy and TS patients and will lead public opinion through their future practice and teaching.
The TS version of the questionnaire appears to be acceptable and there were very few invalid responses. It could therefore be a useful tool for examining knowledge of and attitudes to TS the overall population and internationally as has been done for epilepsy. Such information would provide important information to guide public education strategies in the area of TS and to measure resultant changes in knowledge and attitudes. For TS, just as for epilepsy, "knowledge about the aetiology ... seems to be a very important protector against negative attitudes"7.
In conclusion, knowledge of and attitudes to TS in healthcare students are similar to those for epilepsy. However, widespread ignorance and negative attitudes remain. These may contribute to the comorbidities (such as depression) which as Robertson2 has pointed out are such important determinants of the quality of life of people with TS. As noted by Brook and Boaz4, there is still considerable scope for better education to reduce the stigmatization of people with TS.
References
1. Cavanna A, Schrag A, Morley D, Orth M, Robertson M, Joyce E, et al. The Gilles de la Tourette Syndrome Quality of Life Scale (GTS-QOL) - Development and Validatioon. Neurology 2008; 71: 1410-1416. [ Links ]
2. Robertson MM. The prevalence and epidemiology of Gilles de la Tourette syndrome. Part 2: tentative explanations for differing prevalence figures in GTS, including the possible effects of psychopathology, aetiology, cultural differences, and differing phenotypes. J Psychosom Res 2008; 65: 473-486. [ Links ]
3. Davis KK, Davis JS, Dowler L. In motion, out of place: the public space(s) of Tourette Syndrome. Social Science and Medicine 2004; 59: 103-112. [ Links ]
4. Brook U, Boaz M. Attitude and knowledge of high school pupils towards adolescents with special needs (Tourette's Syndrome). Indian J Pediatr 2006; 73: 1099-1104. [ Links ]
5. Hauser WA, Annegers JF, Rocca WA. Descriptive epidemiology of epilepsy: contributions of population-based studies from Rochester, Minnesota. Mayo Clin Proc 1996; 71: 576-586. [ Links ]
6. Caveness WF, Gallup GH. A survey of public attitudes towards epilepsy in 1979 with an indication of trends over the past 30 years. Epilepsia 1980; 21: 509-518. [ Links ]
7. Spat J, Bauer G, Baumgartner C, Feucht M, Graf M, Mamoli B, et al. Predictors for negative attitudes towards subjects with epilepsy: a representative survey in the general public in Austria. Epilepsia 2005; 46: 736-742. [ Links ]
8. Eddy CM, Rizzo R, Gulisano M, Agodi A, Barchitta M, Calì P, et al. Quality of life in young people with Tourette Syndrome - a controlled study. J Neurol 2011; 258: 291-301. [ Links ]
9. Mula M, Cavanna AE, Critchley H, Robertson MM, Monaco F. Phenomenology of obsessive compulsive disorder in patients with temporal lobe epilepsy or tourette syndrome. J Neuropsychiatry Clin Neurosci 2008; 20: 223-226. [ Links ]
![]() Correspondence:
Correspondence:
Cara Katona
Foundation Year 2 Doctor
University Hospital of North Staffordshire
Newcastle Road
Stoke on Trent, ST4 6QG
United Kingdom
E-mail: cara_p_katona@hotmail.com
Received: 7 June 2012
Revised: 25 November 2012
Accepted: 11 December 2012

