










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Unhealthy lifestyles and increased body weight occur more often in low-socioeconomic status (SES) groups1,2,3,4. Low-SES groups experience systematically worse health or greater risk of illness, a phenomenon called a health differential. The study of the socioeconomic situation can elucidate the mechanisms by which these differentials evolve, resulting in inequities in health, an important component to be investigated in workers’ health2,5,6.
Subjects placed in a low social structure have more material deprivation and restricted access to health services and, therefore, greater susceptibility to the risks of illness1. Furthermore, these individuals are exposed to more harmful working conditions7 and are more likely to have unhealthy habits (for example, lower adherence to exercise) (8,9. In this context, the assessment of isolated risk or protective factors reduces the understanding of the problem instead of clarifying the dynamic interaction of these factors in influencing the health of the population.
Occupational classifications used in epidemiological surveys allow identification of the positive relationship between material resources and health. Occupation may directly interfere with the health status of individuals, due to specific working conditions as physical and ergonomic demands, stress, limited autonomy of decisions and exposure to unhealthy environments. Furthermore, occupations reflect status or social positions, which may be associated with outcomes of nutrition and health according to the opportunities, such as access to healthcare, better education and housing, and healthy foods1,2,10. The occupation, therefore, can interfere in the nutritional status of the individuals, as observed in a study conducted from the National Health Interview Survey - Occupational Health Supplement (NHIS-OHS) in which the prevalence of obesity was higher among health, social assistance and public administration professionals, among others9.
Despite adequate healthy nutrition has been regarded as protective against a series of diseases and mortality, its relation with occupational aspects has been insufficiently studied. Although dietary risk factors can be subject to intervention, they are still treated in isolation in health programs, compromising the effectiveness of their results2,4. It is worth noting, we found no studies examining the presence of multiple risk factors according to occupational status in workers of different occupational status.
Despite the accumulation of knowledge on social inequalities in health, in general, the majority of studies focus on the influence of education or income on health conditions, with little emphasis on dietary habits. To cover this gap, the present study aimed to examine the relationship between nutrition profile and health as well as the coexistence of dietary risk factors according to the occupational status of public municipal employees (temporary and permanent).
MATERIALS AND METHODS
This was an epidemiological survey carried out with public municipal employees of a Brazilian capital between September and December 2009.
All 38,304 public municipal employees (temporary and permanent) of the municipality were invited to participate with the help of the management staff in all agencies of the prefecture through messages on the Internet and intranet and in pay slips and by raising awareness on the importance of participation among the trade unions representing the public municipal employees. Awareness of the research was reinforced in locations with lower adherence when necessary. In total, 5,646 public municipal employees of the municipality (14.7%) answered the questionnaire.
Sociodemographic characteristics investigated include age, sex (female, male), have children (no, yes), marital status (with partner, without partner), in addition to educational level, income, and occupation. Health aspects embraced referred morbidities (Questions: Has any doctor ever told you that you have: systemic arterial hypertension, hypercholesterolemia, diabetes mellitus, or anxiety/depression?), self-assessment of health (Question: Do you classify your health status as? Response options: very good and good; regular, bad, and very bad); referred regular physical activity in the last 3 months (3 times per week).
Self-reported weight and height were used to calculate body mass index, employed in the assessment of nutritional status11 together with habits of monitoring weight and cooking. The consumption of fruits and vegetables (FV), of meat with visible fat and chicken skin was gauged as well as the habit of adding salt to prepared food (except salad). Regarding working conditions and dietary habits, the time available for eating at work, whether or not snacks were offered by the employer, and the presence of a rest room and pantry/canteen in the workplace was queried.
The markers of SES are interrelated, although they are not equivalent. For this reason, we opted to use an occupational status indicator, the International Socio-Economic Index (ISEI), obtained from information on individuals’ educational level, income and occupation, which would allow evaluation of the overall representation of the socioeconomic factors. The ISEI is a scale whose values vary continuously from 16 to 90 points. A higher score is associated with a higher occupational status10.
The Brazilian Occupational Classification was used to obtain the codes of the occupational rating corresponding to the job position plan of the municipality, and was the basis for the calculation of the ISEI. When no match was found for the position within the prefecture, the code that most resembled the function was used, taking into account assignment and competence, minimum required schooling, initial base salary, and place of work. After obtaining the correspondence between the city’s job position and the Brazilian classification, the codes were converted to the Clasificación Internacional Uniforme de Ocupaciones 88 (CIUO88) system using the conversion table available on the website of the Ministry of Work and Employment10.
In this study, the ISEI ranged from 23.0 to 88.0, and for purposes of analysis, was categorized according to tertiles (23.0-30.0, 31.0-51.0, 52.0-88.0), with the initial third corresponding to lower and the final third to higher occupational status.
The organization of data, formation of indicators, and analyses were performed using SPSS 17.0 software for Windows (SPSS Inc., Chicago, IL, USA). The Kolmogorov-Smirnov statistical test was used to check the distribution of continuous variables. Owing to the asymmetrical characteristic of the variables, we chose to present them as median and interquartile range (IR - 25th; 75th percentile).
To verify differences between the variables according to the tertiles of the ISEI values, the χ2 test was used for categorical variables and the Kruskal-Wallis test for participant’s age, adopting a significance level of 5%.
The associations observed were adjusted by the Bonferroni correction to identify possible relationships with each category of ISEI. In the tables, values followed by different letters in the same line are significantly different from each other. After the Bonferroni correction, significant differences were considered when p values were <0.017 [(0.05 (level of significance)/3 (number of groups of comparisons - tertiles of ISEI)].
Whereas inadequate eating behaviors tend to occur simultaneously, increasing the risk of adverse health outcomes, it was evaluated the coexistence of dietary risk factors among the public municipal employees according to tertiles of ISEI. Rectangular Venn diagrams represented these associations graphically. This methodology is based on a graphic display of geometrical shapes that overlap to demonstrate the co-occurrence of certain characteristics of the study population and logical relationships existing between them12. To construct the Venn diagrams, two variables were selected that encompass dietary habits that are associated with the occurrence of non-communicable diseases (NCDs): irregular consumption of FV (an important marker of healthy eating) and ingestion of chicken skin and meat with visible fat (dietary sources of saturated fat)13. In addition to these, we examined reports of insufficient time to eat at work, considered an obstacle to regular meals in a typical schedule, which is one of the pillars of healthy eating.
The participants were informed about the research and access to the questionnaire occurred only after they freely provided informed consent. The study was approved by the Ethics Committee on Research of the Municipal Administration (0054.0.410.000.09ª).
RESULTS
Of 5,646 public municipal employees who answered the electronic survey, 5,090 (90.2%) provided information about variables needed for the construction of the ISEI and were included in the final analysis. The median ISEI value was 38.0 (IR: 29.0; 69.0). In the first, second, and third tertiles of the population, the median ISEI values were 29.0 (IR: 29.0; 29.0), 38.0 (IR: 38.0; 51.0), and 77.0 (IR: 69.0; 85.0), respectively.
The median age of the participants was approximately 42.0 years. There was a predominance of women, which was more pronounced in the low occupational status compared to the highest. Individuals in the lower tertile more frequently reported having children, whereas subjects in the higher tertile more frequently reported having a partner compared with those in the middle tertile (Table I).
Table I Sociodemographic characteristics of public municipal employers, according to ISEI tertiles. Belo Horizonte, MG, 2009.

Note: 1 Values followed by different letters in the same line are statistically different after the Bonferroni correction (p < 0.017); 2 Kruskal-Wallis test; 3 χ2 test. *Total respondents for each variable/category; **Median and interquartile range.
Arterial hypertension and diabetes mellitus were more frequently reported in the low occupational status, whereas hypercholesterolemia was less frequent in the middle tertile. Positive self-reported health was directly related to the occupational status of participants. Regarding the regular practice of physical activity, we identified differences between the more distal tertiles, with a higher percentage of physical activity practice in the higher tertile (Table II).
Table II Health aspects of public municipal employers, according to ISEI tertiles. Belo Horizonte, MG, 2009.
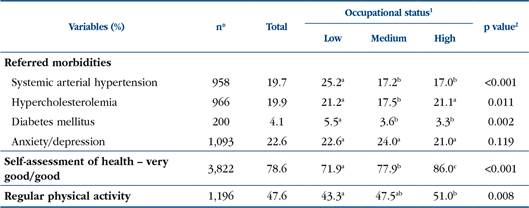
Note: 1 Values followed by different letters in the same line are statistically different after the Bonferroni correction (p < 0.017); 2 χ2 test. *Total respondents for each variable/category.
The frequency of overweight was higher in the group with low occupational status, and the habit of monitoring body weight was higher among the interviewees with higher occupational status. The relationship between cooking habits and occupational status was the opposite. In the higher occupational status group was observed higher frequency of regular consumption of FV (compared with the other two thirds) and lower intake of meat with visible fat or chicken skin (compared with medium third), but they also reported the practice of adding salt to prepared food with greater frequency (compared with the other two thirds). Regarding occupational factors related to dietary habits, the time available to eat during work was lower among the individuals in the higher occupational status group compared with medium occupational status (Table III).
Table III Living habits, nutritional profile and working conditions and dietary habits of public municipal employers, according to ISEI tertiles. Belo Horizonte, MG, 2009.

Note: 1 Values followed by different letters in the same line are statistically different after the Bonferroni correction (p < 0.017); 2 χ2 test; 3 ≥ 6 times per week. *Total respondents for each variable/category.
The Venn Diagram illustrates that for the entire population, 3.0% of employees presented the three-risk factors evaluated (irregular FV intake, meat with fat or chicken skin consumption, and insufficient time to eat at work), without differences among the thirds of ISEI (p=0.942). The overlap of consumption of meat with fat or chicken skin and irregular consumption of FV was the most prevalent combination in the different groups (total population: 19%; low occupational status: 21%; middle occupational status: 19%; high occupational status: 17%). The percentage of workers not exposed to such risks was higher among individuals with high occupational status (p < 0.001) (Figure 1).

DISCUSSION
Differences in eating habits were observed, with a disadvantage for the group with lower occupational status. This group reported unhealthy habits and worse health compared with the group with higher status. Substantiating these findings, the high status group presented the highest percentage of individuals without exposure to dietary risk factors.
The association between the worst health conditions and lower occupational status is in agreement with the literature1,14. Some of the hypotheses that clarify this issue are that these individuals have less adaptive responses to stressors in general, restricted access to health services, worse living conditions, and harmful occupational situations15. Additionally, low socioeconomic levels may favor an unbalanced diet, smoking, and physical inactivity, contributing to the development of NCDs3,4.
Although anxiety/depression is expected in socially disadvantaged individuals16, our results do not confirm this trend. Taking into account the homogeneous nature of the stable standard of employment, we can assume that the negative psychological factors associated with the evaluated comorbidities are homogeneously distributed between the different occupational statuses. In other words, the effects of precarious living conditions that are often determined by unstable employment or unemployment17 would not be modulating the results described in this case.
Some authors have identified a better perception of health in individuals with higher occupational status14. Considered an indicator of health, self-perceived health is commonly used in epidemiological studies as a proxy for the health of individuals. This indicator reflects differences regarding physical activity habits, balanced nutrition, and the strength of family relations among other factors that may interfere with the development of more adaptive coping strategies3,4. It is possible that the results related to health conditions are associated with occupational status; however, it is not possible to fully evaluate this hypothesis.
A larger proportion of individuals with overweight were observed among those with lower occupational status, in agreement with the literature1,2,3,4. Possibly, a lower occupational status is associated with less access to information and limited guidance on weight control, associated with a greater consumption of high-calorie foods compared with lower-calorie foods such as FV, which are considered healthy. In addition, in this dynamic of imbalances, we frequently find a reduced practice of regular exercise3,18,19,20,21. However, a low occupational status was associated with a lower frequency of regular consumption of FV unlike to a greater consumption of fatty foods and less physical activity, which are associated with overweight and NCDs22.
It is worth highlighting that monitoring weight is one of the main strategies for the reduction and long-term maintenance of body weight23. This strategy can function as a positive reinforcement if individuals wish to change their behavior in order to reduce weight and is used as a resource for the prevention and control of overweight in the work environment23,24. However, despite the higher prevalence of overweight among those with lower occupational status, self-monitoring in this group was lower than that in the group with a higher occupational status.
Even though a high occupational status has been related to better dietary habits, the more frequent addition of salt to prepared food, the lower frequency of cooking, and less time to eat during the workday deserves attention. Excessive consumption of salt is related to the development of NCDs. In a study of Japanese workers, a relationship was found between excessive consumption of salt and lower educational level and income25. It is plausible to assume in the present study that not cooking may reflect the possibility of having staff to cook or a greater access to collective food services26. Paradoxically, eating outside the home is common among people with higher income and educational level26.These results deserve the attention of programs that promote healthy eating in the work environment.
Our results indicate that individuals with higher occupational status have less time to for eating during the workday. It is likely that these individuals occupy posts or functions with executive powers. Despite intervals to make the meals are rights of workers, high labor responsibility ultimately constringing them. This is another situation to be targeted by health promotion programs, because restriction of breaks for lunch or snacks can lead to excess eating in subsequent meals as well as inducing the consumption of fast meals at improvised intervals. Overall, these situations favor the intake of high caloric density foods and insufficient chewing, which can impair digestion and satiety22.
Besides the fact that the individuals with higher occupational status report healthier dietary habits, when evaluated in isolation, we observe approximately 30% of the participants in this group were not exposed to any of risk factors, more than the other groups.
Surprisingly, the coexistence of dietary risk factors for NCDs among lower socioeconomic classes27) was not confirmed. The homogeneous nature of the sample in other sociodemographic variables may explain this result. In a study on the overlap of risk factors for cardiovascular diseases among adults in Pelotas, Brazil, around 66% of the population presented two or more behavioral risk factors27. Our results suggest that programs of healthy eating should be presented primarily in group with lower occupational status. Some risk factors for NCD are modifiable, including dietary aspects. A combination of unhealthy behaviors is a predictor of diseases and mortality27,28. The group with higher occupational status is less vulnerable to the events mentioned, with the exception of the time dedicated to eating in the working period.
In addition, a higher proportion of women were observed in the low occupational status group. Despite the gradual insertion of women in the labor market, they are still tending to have worse socioeconomic levels compared to men, which includes receiving lower wages and worse working conditions, exposing them to greater vulnerability to inequities in health related to occupation10.
As our study was of a sample employed and protected as far as social rights are concerned, one should be cautious in comparisons and conclusions. In spite of the stimulus to participate in the research, the response rate was 14.7%, with a greater participation of subjects with more schooling and higher occupational status, and therefore an underestimation of the results is possible. However, it was still possible to evaluate the risk factors for the studied population, characteristics that may be important for the general population. The results obtained are consistent with the state of the art. We found differences between the groups in accordance with their occupational status, reinforcing the importance of the analysis of socioeconomic and occupational conditions when health behavior is assessed.
The number of participants (more than 5,000 employees) in different occupations potentiates the results. The access to this population was made possible by the data collection strategy via the web, which was advantageous owing to its low cost, ease, agility, and long reach within a short time. In this way, we used questions such as self-report of health information and habits to obtain the variables used. While we cannot deny the potential influences of self-reporting bias, self-report is a commonly strategies utilized in surveys and have been associated with a better quality of the respondent replies29.
The use of the ISEI enabled the development of a marker that incorporates various dimensions of the socioeconomic situation, which is an advantage with respect to the exclusive use of the income variable or of the education variable when health conditions are investigated30. The analysis of the coexistence of dietary risk factors, using a Venn diagram, increased the advantages mentioned by allowing the examination of multiple aspects involved in chronic comorbidities prevalent in Brazilian adults.
In this study, even though only employed individuals were evaluated, with consequent homogeneity of the sample in this aspect, relevant socioeconomic differences were observed, which may be related to the determination of inequities in health. Although reducing these inequities is an important goal in terms of public health, the majority of programs aimed at workers’ health have not yet focused on individuals of lower occupational levels, which may be contributing to the maintenance of inequalities1. Thus, the implementation of intersectoral actions is essential for the implementation of structural changes, and it is especially important the joint work of public health and occupational health agents in order to promote the health potential of populations.
The results presented here display a relationship among the dietary profile and health conditions and occupational status of public employees and demonstrate a disadvantage for those with lower occupational status. Such findings indicate the need for public policies for the promotion of health, with a special focus on nutrition. The working environment is a privileged space to carry out educational activities with scope for improving the nutrition and health of different social groups. However, the singularities related to socioeconomic conditions must be taken into account when the objective is to ensure equity in health. Thus, additional studies in different populations of workers would be useful to deepen the understanding of the mechanisms that relate occupational status to health and nutrition.

