










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.98 no.2 Madrid feb. 2006
IMAGES IN DIGESTIVE PATHOLOGY
Epiploic appendicitis
F. J. de Castro García, J. A. Santos Sánchez1, P. García Iñigo1 and J. C. Díez Hernández1
Service of Radiodiagnosis. Hospital Ciudad de Coria. Cáceres, Spain. 1Hospital Universitario de Salamanca, Spain
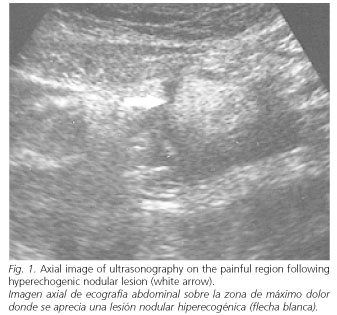
The present case describes a 23-year-old woman with no pathological history of interest. The patient presented with 48-hour-standing supraumbilical abdominal pain in the absence of disturbed intestinal rhythm, nausea, sickness or dysthermic sensations. Her last menstruation had taken place 5 days prior to the onset of disease. The patient was alert and oriented during the course of the physical exploration. She had febricula (37.5 ºC) and tenderness in the supraumbilical region, with signs of peritoneal irritation at the same level. Murphy and Rovsing signs were negative. A laboratory workup revealed a leukocyte count of 12,200 with 80.5% neutrophils. C-reactive protein was 21.80 (0-1). All the remaining laboratory parameters were within normal limits. No alterations were seen on abdominal X-ray films. On suspecting a strangulated epigastric hernia, an abdominal ultrasonography was performed (Fig. 1), following which a hyperechogenic lesion, delimited by a hyperechogenic ring surrounded by a small amount of fluid, was seen in the painful region.
An abdominal CT was performed (Fig. 2) focused on the pathological zone using no intravenous or oral contrast material, during which the presence of a rounded mass with a density slightly higher than that of the adjacent fat tissue, and with a hyperdense central area was confirmed. Considering the severity of pain and the presence of signs indicating local peritoneal irritation, the patient was operated upon, and a torsion of the epiploic appendix was seen and solved by a partial resection of the greater omentum. The patient evolved favourably, and her abdominal manifestations remitted.

The omentum is a free fold of peritoneum formed by the latter's union with the anterior and posterior lining of the stomach. Epiploic appendices are small peritoneal prolongations, under 5 cm in size, which contain several vessels and fat, located on the serosal surface of the colon from the cecum to the rectal-sigmoid junction. Both structures may occasionally develop an infarction as a result of torsion or spontaneous venous thrombosis, which is usually designated as omental torsion or epiploic appendicitis, depending on whether the omenta or epiploic appendices have been involved (1).
The incidence of this complaint is 3-7% in patients with suspected acute diverticulitis, and 1% in patients with pain in the right fossa iliac (2).
Clinically speaking, it tends to manifest as abdominal pain and abdominal tenderness with a variable distribution, although it is most common in the lower quadrants (3). It may be accompanied by febricula. From a laboratory viewpoint, leukocyte counts are normal or slightly high, usually accompanied by increased C-reactive protein levels.
The ultrasonographic study revealed a round or oval, non-compressible echogenic mass beneath the area of maximum pain (4). This finding is characteristic of what is known as "intraabdominal focal fat infarction", which includes both epiploic appendicitis and omental infarction (5). Differential diagnosis between the aforementioned conditions is based on CT imaging characteristics, basically the presence of a hyperdense central area, which in histological terms represents the torsion of the appendix (2,4).
The correct management of these patients relies on both an adequate diagnosis and analgesic therapy, as it is recommended that surgery be restricted to cases presenting with complications or severe pain resistant to other treatments (5).
References
1. Tolenaar PL, Bast TJ. Idiopathic segmental infarction of the greater omentum. Br J Surg 1987; 74: 1182.
2. Mollá E, Ripollés T, Martínez MJ, Morote V, Roselló-Sastre E. Primary epiploic appendagitis: US and CT findings. Eur Radiol 1998; 8: 435-8.
3. Levret N, Mokred D, Quevedo E, Barret F, Pouliquen X. Les appendicitis epiploïques primitives. J Radiol 1998; 79: 667-71.
4. Rioux M, Langis P. Primary epiploic appendagitis: clinical, US, and CT findings in 14 cases. Radiology 1994; 191: 523-6.
5. Van Breda Vriesman AC, Lohle PNM, Coerkamp EG, Puylaert JBCM. Infarction of omentum and epiploic appendage: diagnosis, epidemiology and natural history. Eur Radiol 1999; 9: 1886-92.

