










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.98 n.6 Madrid Jun. 2006
ORIGINAL PAPERS
Public opinion survey after capsule endoscopy: patient's point of view on its utility
Encuesta de opinión tras estudio con cápsula endoscópica: percepción de su utilidad por el enfermo
B. Velayos, L. Fernández, R. Aller, F. de la Calle, L. del Olmo, T. Arranz and J. M. González Hernández
Service of Digestive Diseases. Hospital Clínico. Valladolid, Spain
ABSTRACT
Aim: when programming a medical test such as capsule endoscopy (CE), finding the closest point between the patient's experience and his/her expectation is essential to improve any further explorations.
For this purpose we designed a form which tries to collect the information required.
Material and methods: from December 2003 to January 2005 we examined the small intestine of 98 patients with the help of CE. Later they were sent an anonymous questionnaire in July 2005, which included 10 questions upon the origin and previous knowledge of the patient about this technique, their tolerance to it, and the value they attached to it with regard to finding a new diagnosis and assigning different treatments, and also the incidence in the positive or negative evolution of their disease in particular and of medicine in general.
Results: answer rate reached 58% and was slightly higher among women and people over 70 years; 80% of repliers had been informed about CE by a physician, while nearly all the rest had received previous information from the media; 37% had had symptoms for more than 12 months, while only 17% had suffered them for one month before the exploration. A bit over 30% did not know what the specific diagnostic field of the test was (most of them women and young people), although most of them were not surprised by the procedure. Over 75% showed "acceptable" or "excellent" tolerance, while 5.5% (most of them young people) found it hard to bear. The opinion about its utility in the diagnosis was 37%, and although 70% thought that CE had revealed nothing new about their pathology, over 60% declared feeling better after the test; 84% pointed out that it had achieved a breakthrough for their quality of life (most of them men and very old people), and only 13% thought it was worthless. However, nearly all the answers agreed in that CE was an "important" or "very important" diagnostic device.
Conclusions: after the test using CE, the diagnostic benefit detected by the patient is not the same as that shown by technical studies. Nevertheless, the test can be highly satisfactory for the patient in particular, and also in an overall view.
CE is a well-tolerated test, applied in our setting to chronic diseases and that, contrary to what we supposed, is explained to patients mainly by a physician. Most of them are not familiar with its specific indications.
Key words: Capsule endoscopy. Public opinion survey. Tolerance.
Introduction
Public opinion surveys are mainly intended to give professionals and healthcare representatives the necessary information about patient degree of satisfaction with regard to services they receive. In a society where the rise in medical care quality by means of modifying different scopes in the process of attendance is especially esteemed (1), approaching the patient's point of view about what can be improved is vital when programming different techniques (2), especially those recently introduced.
The study of small intestine pathologies has shown a remarkable evolution since we started using CE, which was officially approved in 2001 by the FDA; from that very year it has been a subject of publication in our country (3,4). The aforementioned device, after being swallowed by the patient, runs along the gastrointestinal tract taking two photographs per second during the 7 or 8 hours its trip lasts (5). The new approach that CE offers to the small intestine, together with its scarce contraindications, absence of radiation, and minimum number of complications (reduced to obstruction) allows to use it for new indications and has turned it into a usual diagnostic instrument in our field (6,7). The fact that it is usually the last step in the diagnostic process helps the patient think that the technique itself and everything around it is not very complicated. However, carrying out this test implies a procedure that requires accurate medical and administrative coordination, as well as being aware of patient expectations regarding the exploration, potential incidents, and the help it could offer in treating their diseases or progressing in their diagnosis.
As a result of that concern not only for technical and scientific issues, several studies, though not specifically aimed, have included questions to assess patient opinions after CE (8,9). In any case, and maybe because it is a recent test, no studies clearly show the level of information, tolerance, satisfaction and usefulness detected by the patient after being tested with CE.
Although public opinion surveys have the drawback that users tend to express socially accepted answers (10), their relevance is agreed on by most professionals and health authorities (2). Thus, we sent a straightforward questionnaire to all patients who had been tested with CE at least 6 month before, probing mainly patient knowledge on the test, tolerance, and personal opinion on its value regarding the positive or negative evolution of their pathology and of medicine at large.
Material and methods
From December 2003 to January 2005 we used CE to study the small intestine of 98 patients in our area, which includes the Autonomous Community of Castile and Leon (2.5 million inhabitants). The total number of explorations was 100, with repeats on the same subject twice, and a number of severe complications of 1. Applications were always made by physicians, most of them gastroenterologists, followed by internists, surgeons, and hematologists.
After receiving the form, which always enclosed a record including clinical assessment and health insurance data, we telephoned every patient to tell him/her when they should come to our department. By that day, they had received information with some basic details about the test, such as the need of coming with somebody else, wearing loose clothes, following a liquid diet the day before, etc., as well as the possibility of having a light snack 4 hours after the beginning and the warning of avoiding electronic devices together with the need of informing us about either any incidents or non-expulsion after 4 days. We did not use prokinetics or solutions for cleaning the intestine in any of them. We required the signing of an informed consent. We always used the same system "Given Imaging M2A plus®" with a situation localizer through 7 sensors placed per protocol on the abdomen, a recording system "Data Recorder TM Given®" (weighing about 200 grams), and external nickel batteries (1 kg). The last two devices were placed in a special belt "RecorderBeltTM" (Fig. 1). The capsule ("M2A plus®"), which was swallowed with water, weighs 3.45 g and its dimensions are 26 x 11 mm. The viewing of recordings was usually carried out in a few days (the same evening in cases with severe active bleeding), always sending a report to the applicant doctor within 2-4 weeks.

As for sex distribution men represented 58.16% of the survey, and the average age was 59.67 years (ranging from 15 to 87 years); 13.27% of patients were under 40 years, 46.94% were over 40 and under 70, and 39.80 were over 70. Regarding indications, three out of four tests were aimed at completing a study for obscure digestive bleeding; suspicion of potential inflammatory bowel disease occurred in 1 out of 10 cases, while the search for celiac disease or tumors/polyps in the small intestine was hardly representative.
The diagnosis obtained consisted mainly of vascular disorders (in half of procedures), no relevant finding (2 out of 10), and suspicion of Crohn's disease (in a bit over 1 out of 10 tests), while finding tumors-polyps, damage with an inconclusive diagnosis, blood without injury, or diffuse enteropathy in approximately 5% of cases in each of the above-mentioned categories.
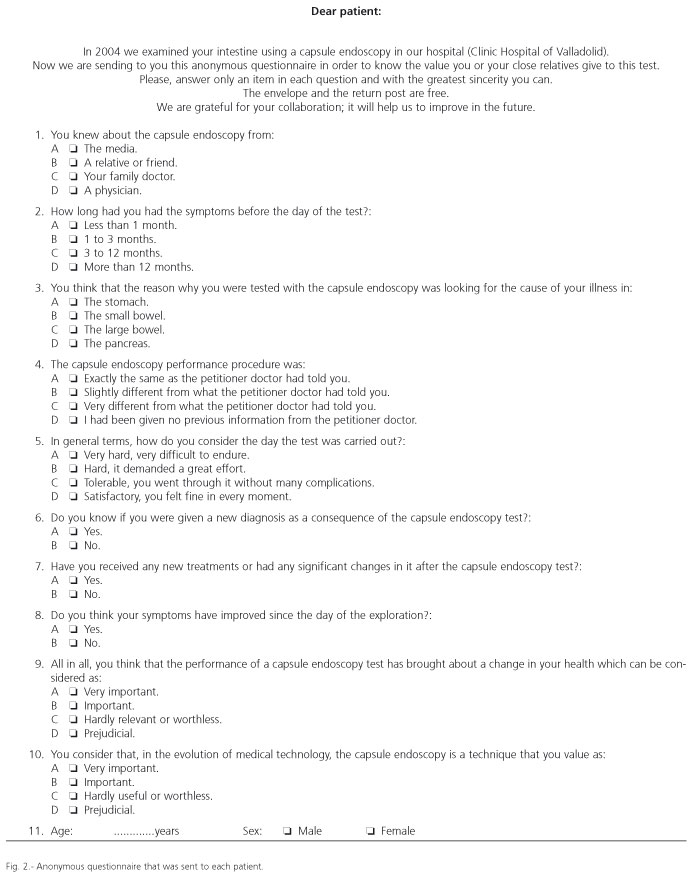
During the first week of June 2005, our Hospital's Admission Dept. posted a 10-item questionnaire to patients who had been tested with CE 6 months before -7 questions had 4 possible answers and 3 had only 2 options; the anonymous nature of the questionnaire as well as the need of choosing only one option per question were explained (Fig. 2). We enclosed a stamped envelope with our department address printed on it. The survey's deadline was December 1st, 2005.
Results
When we met the deadline we had received 54 replies and 5 letters had been returned (2 of which were from male patients aged 81 and 71 who had died, while the other 3 were 2 males and 1 female who had not been found by the mail service). All questionnaires collected had a mark in at least one of the boxes except for 2 males who had only answered 2 and 8 of the questions. Just on 3 occasions we noticed more than one answer in a question: 1 of them was a triple answer and the other 2 were double responses, always answering question 3.
In conclusion, total answer rate reached 55.1% (54/98), which rises to 58.06% (54/93) if we just count the patients who supposedly received the application form. Half of them corresponded to each sex, though answer rates were higher among women (69.23%, 27/39) versus men (50%, 27/54).
As for age (the second epidemiologic parameter required), there was no difference in average age for the total number of patients tested with CE (59.70 years, repeating the same range: 15-87 years), while sex differences were no significant with an average age of 59.44 years in males (15-87 years) and 57.96 years in females (18-83 years). Responders also showed an age distribution similar to that in the total number of patients who were sent the questionnaire, this being 12.96% (7/54) under 40 years, 44.44% (24/54) between 40 and 70 years, and 42.59% (23/54) at 70 or over. The highest answer rate corresponded to the third group (65.71%, 23/35), while the rate in the group involving the youngest people reached 58.33% (7/12), and the middle-aged group obtained 52.17% (24/46).
For each of the 10 questions, the total percentage of answers that each option revealed, as well as its division according to sex or age, resulted as follows (NA: not answered):









Discussion
The present models that try to improve the quality parameters of various explorations tend to take into account not only the technical competence but also the humane side, considering patient perception (11). It is known that satisfaction with a medical test depends on the proximity between personal experience and expectancies (12). Factors that can rise the level of a healthcare service, apart from medical results, derive from tangibility, reliability, interest, guarantee and empathy levels in patients. We may also consider essential other factors such as competence, politeness, communication, trust, security, access and information (11).Although in our setting we have carried out a lot of studies using different methods to try and value how the patient observes his/her medical condition (13), not many of them focus on an endoscopic technique in particular (14) and the way in which it influenced their quality of life. CE, broadly followed by mass media in our country (15-18), is nowadays a mainstay in the study of small intestine pathologies and, in spite of generating so many reflections, none has come across the patient's outlook in depth. Moreover, there are hardly any publications about the outcome of people explored (19).
In our approach, the first thing that draws our attention is the answer rate, similar or higher to that of other written surveys (20,21), nearly reaching 60%, being clearly higher among women. It is the group including the oldest people where the repliers´ rate approaches telephone surveys (near 70%).
Analyzing the most important points in every question of the survey, we have to point out that most patients (more than 80%) declared having learned about CE through a physician's accounts (especially women and people over 70 years of age), while nearly all others had obtained information via the mass media. In a society where some medical news (particularly those concerning new methods such as the CE) seem to reach the vast majority of the population (15,22), the fact that less than 15% of the polled people knew about its existence through the media can be an issue when performing tumor screening programs, vaccinations, health campaigns, etc. The complexity of diseases related to the small bowel may have taken away the relevance of the family doctor.
The period of time with symptoms which patients referred to in the second question, stated that the performance of CE tests in our first cases occurred mainly in chronic situations, especially in men and middle-aged people. Among women and patients over 70 years of age it was carried out for more severe pathologies. Our waiting list has never been longer than one month, so we should attribute the results to other factors such as underlying disease, study complexity in those patients, delay in filing the application, etc. Publications on the benefits of CE regarding symptom outcome over time have stated the great advantage of its use on subjects with recent symptoms (23). On the other hand, and before CE, the diagnosis of injuries causing obscure bleeding in the small bowel was finally achieved after an average of 2 years (range 1 to 8) (24).
A bit over 30% of surveyed people did not know what the diagnostic field of CE was, and women were interestingly absolutely ignorant in this respect among patients under 40 years of age, while middle-aged patients were best informed. This is in contrast to reports from most of them that they were not surprised by the CE procedure -we presume that the information leaflet we sent them helped, although, to tell the truth, in that leaflet they were also told about the place in the intestine that we were going to explore, and 13% reported having no information, especially women and aged patients. According to these data and supporting CE as a well-tolerated test (25), more than three quarters marked it "good" or "excellent" (men in a higher proportion), with just 5.5% finding it hard to bear. The worst data with regard to this subject were those obtained from women and young patients (who, oddly, had found it hard to bear in nearly 30% of cases). In no cases the use of prokinetics or laxatives was considered (26), something which might have changed these results. Even so, the evacuation rate reached 90% (27).
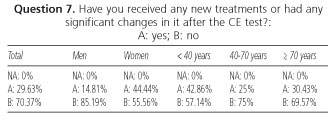
Opinions about its utility did not come up to the diagnostic efficiency we achieved in our series (close to 80%) and published in several studies and reviews (these reached acceptance over 65%) (28-30), and it reached a new, previously unknown diagnosis in 37%. This percentage is higher in women and patients under 40 years, while clearly under average in men and patients from 40 to 70 years of age. We also found out that they were more aware that after CE they had received treatment that was different to the initial one in the same groups (women and young patients), and although 70% believed that the test had offered no new information about their diseases, a bit over 60% of the patients who answered the survey admitted feeling better, with no difference in sexes and directly related to age. It is not easy to ascertain whether a lack of communication between the applicant doctor and the patient helps justify this discord somehow.
Figures showing good tolerance, acceptance and trust in the technique are supported by the supposition of 84% of patients that CE meant a "very important" or "important" step forward to improve their quality of life, being men and the 2 groups involving both young and old patients where this opinion was most widely backed. Just 13% of them thought the benefit they had obtained with the test was worthless (in spite of their answers to questions 6, 7 and 8), an opinion that was not argued with criticism or negative reflection when questioned about the utility of CE in general (98% scored the method as an "important" or "very important" medical device). The greatest degree of satisfaction came from those who had improved their medical condition, although these were not the subjects who obtained more information regarding new diagnoses or treatments derived from the exploration.
We are aware of the difficulties entailed in setting up a methodology to measure the different perceptions of patients, and even more in trying to level practice up to patient expectancies (31). Future reflections should also take into account information from applicant doctors and look into not only personal opinions but also the ability of CE to avoid stays in hospitals, transfusions, medical complications or sick leaves. As Castile and Leon is a scattered-population area, we have had difficulties to get such information. Although the size and epidemiology features of our series are similar to those of others, indications do not share a similar variety (32), with most of them corresponding to obscure digestive bleeding (33,34).
In the light of the data collected from the expounded public opinion survey we may conclude that the diagnostic benefit perceived by patients tested with CE is smaller than what our technical competence studies show, causing a poor opinion on its utility when they refer to changing their baseline treatments. However, the test can elicit great acceptance and satisfaction in the patient considering their particular case, giving it an outstanding relevance in the setting of medical technology. It is a well tolerated exploration used in our field to study long-lasting diseases and that, contrary to what we could believe due to its presence in the media, is known mainly through physician accounts. Even so, a lot of patients ignore what it is used for -that is, to explore parts of the small intestine which would be otherwise inaccessible.
Acknowledgements
The authors thank to Mr. Félix Lozano, and Ana Almaraz, MD for their collaboration and help.
References
1. Vuory H. Patient satisfaction, an attribute or indicator of the quality of care? QRB 1987; 13: 106-8. [ Links ]
2. Maderuelo JA, Carriedo E, Serrano M, Almaraz A, Berjón AC. Factores de insatisfacción con la asistencia sanitaria. Un estudio Delphi. Atención Primaria 1996; 17 (5): 348-52. [ Links ]
3. Pérez Piqueras J, Payeras G. Cápsula endoscópica. Gastroenterología Integrada 2001; 2 (1): 44-7. [ Links ]
4. Barroso N, Caunedo A, Rodríguez M, Herrerías Esteban JM, Pellicer F, Herrerías Gutiérrez JM. Cápsula endoscópica. Rev Esp Enferm Dig 2001; 93 (9): 598-601. [ Links ]
5. Given Imaging Limited. Sistema de diagnóstico Given®. Manual del usuario RAPID®2. Versión Español. Given Imaging Limited. Israel 2001-2. [ Links ]
6. Reunión de Consenso de la AEED y SEPD sobre Aplicaciones Clínicas de la Cápsula Endoscópica. Marbella, junio del 2003. [ Links ]
7. Balanzó J, González B, Sáinz S. Cápsula endoscópica: presente y futuro. Gastroenterol Hepatol. 2002; 25 (4): 251-3. [ Links ]
8. Petroniene R, Dubcenco E, Baker JP, Ottaway CA, Tang SJ, Zanati SA, et al. Endoscopia con la cápsula Given® en la enfermedad celíaca: evaluación de la exactitud diagnóstica y del acuerdo entre observadores. Am J Gastroenterol (Ed Esp) 2005; 2: 167-76. [ Links ]
9. Leighton JA, Srivathsan K, Carey EJ, Sharma VK, Heigh RI, Post JK, et al. Safety of wireless capsule endoscopy in patients with implantable cardiac defibrillators. Am J Gastroenterol 2005; 100: 1728-31. [ Links ]
10. Chacón F. Los estudios sobre satisfacción de los pacientes: una aproximación crítica. Jano 1990; 38: 1117-23. [ Links ]
11. Bowers MR, Swan JE, Koehler WF. What attributes determine quality and satisfaction with health care delivery? Health Care Manage Rev 1994; 19 (4): 49-55. [ Links ]
12. Asadi-Lari M, Tamburini M, Gray D. Patient's needs, satisfaction, and health related quality of life: towards a comprehensive model. Health and quality of life outcomes 2004; 2: 32. [ Links ]
13. Díaz-Rubio M, Moreno-Elola C, Rey E, Locke GR. Symptoms of gastro-oesophageal reflux: prevalence, severity, duration and associated factors in a Spanish population. Aliment Pharmacol Ther 2004; 19: 95-105. [ Links ]
14. Sola-Vera J, Esteve MD, Gutiérrez A, García MF, Mozos G, Girona E, et al. Actitud del paciente ante la información y el consentimiento informado en endoscopia digestiva. Resultados de una encuesta de opinión. Revista de la Sociedad Valenciana de Patología Digestiva 2001; 20 (3): 114-5. [ Links ]
15. Rodríguez A. Viaje al interior del ser humano. El Mundo, Suplemento de Salud, 13 de julio del 2002. [ Links ]
16. El Norte de Castilla, 23 de mayo del 2004. P6. [ Links ]
17. Diario de Ávila, 20 de febrero del 2005. P20. [ Links ]
18. Diario de Burgos, 20 de febrero del 2004. P33. [ Links ]
19. Saurin JC, Delvaux M, Vahedi K, Gaudin JHL, Villarejo J, Florent C, et al. Clinical impact of capsule endoscopy compared to push enteroscopy: 1 year follow up stydy. Endoscopy 2005; 37 (4): 318-23. [ Links ]
20. Vaquer JV, Ponce J, Vegazo O, Palacios A, Sofos S, Zapardiel J, et al. Grupo del Estudio IBERGE. ERGE en España: prevalencia, factores de riesgo asociados y calidad de vida. Comunicación oral. VII Congreso Nacional de la AEG. Madrid, 2004. [ Links ]
21. Casellas F, Fontanet G, Borruel N, Malagelada JR. Opinión de los pacientes con enfermedad inflamatoria intestinal sobre la atención sanitaria recibida. Rev Esp Enferm Dig 2004; 96 (3): 174-84. [ Links ]
22. Jauregui P. Una cápsula permite obtener imágenes del sistema digestivo. El Mundo, Suplemento de Salud. 27 de mayo del 2000. [ Links ]
23. Pennazio M, Santucci R, Rondonotti E, Abbiati C, Beccari G, Rossini FP, et al. Outcome of patients with obscure gastrointestinal bleeding after capsule endoscopy. Report of 100 consecutive cases. Gastroenterology 2004; 126 (3): 643-53. [ Links ]
24. Sahai A. An assessment of the use of costs and quality of life as outcomes in endoscopio research. Gastrointest Endosc 1997; 46 (2): 43-8. [ Links ]
25. Fleischer DE. Capsule endoscopy: the voyage is fantastic. Hill it change what we do? Gastrointestinal Endosc 2002; 56: 542-6. [ Links ]
26. Cos E, González C, Menchén L, Núñez O, Ponferrada D. Estado actual de la cápsula endoscópica. Actualizaciones temáticas Madaus. Editorial Glosa, Barcelona 2004. [ Links ]
27. Velayos B, Fernández L, Aller R, De la Calle F, Del Olmo L, Arranz T, et al. Estudio de los tiempos de tránsito gastrointestinal con cápsula endoscópica. Gastroenterol Hepatol 2005; 28 (6): 315-20. [ Links ]
28. Saurin JC, Delvaux M, Gaudin JL, Fassler I, Villarejo J, Vahedi K, et al. Diagnostic value of endoscopic capsule in patients with obscure digestive bleeding: blinded comparison with video push-enteroscopy. Endoscopy 2003; 35 (7): 576-84. [ Links ]
29. Mata A, Bordas JM, Feu F, Ginés A, Pellise M, Fernández-Esparrach G, et al. Wireless capsule endoscopy in patients with obscure gastrointestinal bleeding: a comparative study with push enteroscopy. Aliment Pharmacol Ther 2004; 20 (2): 189-9. [ Links ]
30. Caunedo A, Rodríguez-Tellez M, Barroso N, García JM, Pellicer FJ, Herrerías JM. Papel de la cápsula endoscópica en el manejo del paciente con hemorragia digestiva de origen oscuro. Rev Esp Enferm Dig 2002; 94: 482-7. [ Links ]
31. Sofaer S, Firminger K. Patient perceptions of the quality of health services. Annual Rev of Public Health 2005; 26: 513-59. [ Links ]
32. Caunedo A, Rodríguez-Téllez M, García-Montes JM, Gómez-Rodríguez BJ, Guerrero J, Herrerías JM Jr, et al. Utilidad de la cápsula endoscópica en pacientes con sospecha de patología de intestino delgado. Rev Esp Enferm Dig 2004; 96: 10-21. [ Links ]
33. Vázquez-Iglesias JL. Cápsula endoscópica: una nueva etapa en la historia de la endoscopia. Rev Esp Enferm Dig 2004; 96: 3-9. [ Links ]
34. Balanzó J, González B, Sáinz S. Cápsula endoscópica: presente y futuro. Gastroenterol Hepatol 2002; 25 (4): 251-3. [ Links ]
![]() Correspondence:
Correspondence:
B. Velayos.
Servicio de Enfermedades Digestivas.
Hospital Clínico.
Avda. Ramón y Cajal, 3.
47011 Valladolid
e-mail: benitovelayos@hotmail.com
Recibido: 22-09-05
Aceptado: 25-03-06

