










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.98 no.9 Madrid sep. 2006
PICTURES IN DIGESTIVE PATHOLOGY
Small-bowel intussusception secondary to metastatic melanoma
Invaginación intestinal asociada a metástasis de melanoma maligno
E. M. López-Tomassetti Fernández, J. Pérez-Palma and A. Carrillo Pallares
Department of Gastrointestinal Surgery. Hospital Universitario de Canarias. Santa Cruz de Tenerife. Spain
A 39-year-old woman was referred to our department in June 2004 with a 1-month history of anemia, recurrent abdominal pain, and abdominal distention. She had had a malignant melanoma excised from her back with a sentinel node biopsy in the axilla, which was considered positive for micrometastases (June 2003); the patient received Kirkwood interferon-a2b adjuvant therapy for one year with good tolerance.
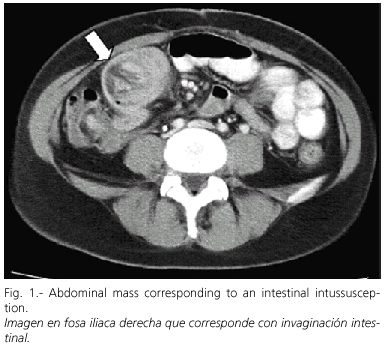
Abdominal ultrasounds revealed a mass in the right iliac fossa, and a CT scan showed submandibular nodes as well as small-bowel intussusception at the ileum, with a large nodular tumor in this same site (Fig. 1). A surgical exploration was decided upon. Laparotomy revealed intussusception of the lower ileum (Fig. 2b.), which was caused by multiple large polypoid lesions (Fig. 2a) accompanied by enlarged mesenteric lymph nodes. We performed a right hemicolectomy and resected 70 cm from the affected small bowel and involved mesentery, followed by a side-to-side ileocolic stapled anastomosis. The pathology report confirmed the presence of various exophytic polypoid tumors partially occluding the lumen, which were invading the submucosa. Mesenteric lymph nodes were also invaded by the same tumor, which proved to be a metastatic melanoma (positive for S-100 and HMB-45).
Although the gastrointestinal (GI) tract is an uncommon site for metastasis, melanoma is one of the most common tumors to metastasize to the GI tract. Only 2 to 4% of patients with melanoma will be diagnosed with GI metastases during the course of their disease. Most authors recommend surgical resection for melanoma that is metastatic to the GI tract as it provides a significant improvement in quality of life with low operative morbidity and mortality (1). When no extra-GI disease exists and a complete resection can be accomplished, long-term survival may be achieved in a minority of patients.
Ricaniadis et al. reported a study of 47 patients who underwent resection for metastatic melanoma to the GI tract. Median survival was 28 months for patients having undergone complete resection, compared to 5 months for patients having undergone incomplete resection (2).
etastatic lesions from malignant melanoma may have different pathological patterns: polypoid (most common), cavitary, infiltrating, and exoenteric. Small-bowel lesions can present with bleeding, anemia, vague abdominal pain, an abdominal mass, and weight loss, or may remain asymptomatic until bowel obstruction occurs, most often from intussusception (3). Any patient with melanoma and GI symptoms or chronic blood loss should undergo abdominal ultrasonography and computed tomography evaluations of the alimentary tract (4).
References
1. Manola J, Atkins M, Ibrahim J, Kirkwood J. Prognostic factors in metastatic melanoma: a pooled analysis of Eastern Cooperative Oncology Group trials. J Clin Oncol 2000; 18 (22): 3782-93.
2. Ricaniadis N, Konstadoulakis MM, Walsh D, Karakousis CP. Gastrointestinal metastases from malignant melanoma. Surg Oncol 1995; 4 (2):105-10.
3. Bender GN, Maglinte DD, McLarney JH, Rex D, Kelvin FM. Malignant melanoma: patterns of metastasis to the small bowel, reliability of imaging studies, and clinical relevance. Am J Gastroenterol 2001; 96 (8): 2392-400.
4. Gaffke G, Stroszczynski C, Schlecht I, Jost D, Ludwig WD, Schlag PM, Felix R. Diagnosis of tumors of the small intestine with the aid of CT contrast enema. Sellink CT technique evaluated in 63 patients. Rontgenpraxis 2002; 54 (6): 214-9.

