










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.99 n.9 Madrid Sep. 2007
Retrorectal tumors: Excision by transanal endoscopic microsurgery
Tumores retrorrectales: excisión por microcirugía endoscópica transanal
S. Zoller, A. Joos, D. Dinter!, W. Back2, K. Horisberger, S. Post and P. Palma
Departments of Surgery 1Radiology and 2Pathology. University Hospital Mannheim. Germany
RESUMEN
Los tumores del espacio retrorrectal representan una patología poco frecuente. Debido a su singularidad incluida la amplia sintomatología con la que debutan, son a veces causa de diagnósticos y tratamientos erróneos.
Esta nota clínica informa sobre tres casos surgidos en mujeres con variada sintomatología donde se incluía dolor rectal, enfermedad supurada anal recidivada y estreñimiento. La masa retrorrectal fue diagnosticada tras exploración clínica y pruebas de imagen donde se incluía ecografía endorrectal, resonancia magnética y endoscopia.
La exéresis quirúrgica se realizó mediante microcirugía transanal endoscópica, en un intento de combinar una visualización mejorada de la disección y una técnica mínimamente invasiva. La anatomía patológica demostró en los tres casos quistes caudales. Esta nota clínica describe por primera vez en la literatura la resección quirúrgica de tumores localizados en el espacio retrorrectal mediante microcirugía transanal endoscópica.
Palabras clave: Micricirugía transanal endoscópica. Tumor retrorrectal.
ABSTRACT
Tumours within the retrorectal space are uncommon. Due to their rarity and diverse symptoms they are often misdiagnosed or mistreated.
We report three cases of women presenting a variety of symptoms including increased rectal pain, recurrent abscesses/fistulas and constipation. Upon clinical examination and further investigations using MR scan, endorectal ultrasound and endoscopy, a retrorectal mass was suspected in all three cases.
In order to achieve a complete excision of the tumor while minimizing trauma, transanal endoscopic microsurgery (TEM) was performed. The histology of the multicystic tumor revealed in all three cases a tailgut cyst. As far as we know this is the first report describing the use of TEM for surgical treatment of tumors located in the retrorectal space.
Key words: Transanal endoscopic microsurgery. Retrorectal tumor.
Introduction
Retrorectal tumors are rare entities predominantly seen in adult women. Within the retrorectal space different types of tissue may give rise to benign or malignant growth. Two thirds of these lesions are of congenital origin, e.g., tailgut cysts, which are also known as postnatal gut cysts or retrorectal cyst hamartomas. Reviewing the literature most of the cases are asymptomatic, especially benign ones, frequently found on routine complete physical examination (1-4). If present, reported symptoms include chronic perineal pain and complaints referring to mass effects like low back pain and chronic weakness in the legs. Complaints of constipation, caused by interference with the passage of stool, or feeling of unsatisfied defecation are also mentioned in the literature. Due to its rarity, tailgut cysts are often misdiagnosed or mistreated. Usually the lesions are circumscribed, unencapsulated and multicystic. Histological diagnostic criteria include the presence of various types of epithelia of the congenital gut without a well-defined muscle cell layer or a myenteric plexus. Complete excision is required because of the risk of recurrence, infection and malignant transformation. Operative approaches include the abdominal, posterior or transanal method.
In the following we report three cases of tailgut cysts occurring in women complaining about recurrent abscesses and constipation. The retrorectal cyst was treated by means of transanal endoscopic microsurgery (TEM).
Presentation of the cases
Case 1
A 49-year-old female with a 10-month history of increasing rectal pain and recurrent retrorectal abscesses was transferred to our colorectal unit. Upon admission and digital rectal examination a moderately tender mass was assessed in the retrorectal space. The endoscopy showed an extrinsic compression of the rectum without mucosal changes.
MR scan (Fig. 1) was performed, presenting a fluid-filled cystic mass posterior to the rectum. Suspecting a congenital cyst at this point, a complete surgical excision of the mass using transanal endoscopic microsurgery was carried out.

Intraoperatively, several cystic lobules were identified with adhesions to the retrorectal space. Blunt and sharp dissection was used to separate the mass from the presacral space. During dissection, one cyst-compartment was entered and produced large amounts of an opaque and grey fluid.
The histopathological examination of the cystic lesion showed a tailgut cyst and demonstrated multiple cysts lined by cylindrical, mucus secreting as well as multi-layered squamous epithelium. These cysts were surrounded by dense fibrous tissue and poorly formed smooth muscle. There was no evidence of malignancy. The postoperative course was uneventful.
Case 2
A 55-year-old female with a 24-month history of recurrent anal fistula and abscesses was admitted. Inspection and digital rectal examination revealed a tumor of the retrorectal space. Because of the multiple fistula-in-ano surgery a MR was indicated. A retrorectal tumor was suspected as the origin of the recurrent abscess formation and transanal endoscopic microsurgery was scheduled. The intervention and postoperative course were uneventful (Fig. 2). The histopathological examination of the cystic lesion confirmed a tailgut cyst.

Case 3
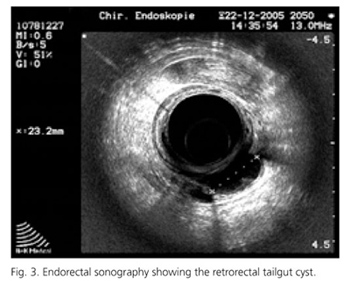
A 51-year-old female with a 9-month history of increasing rectal pain and constipation was referred to our university hospital. Clinical investigation upon admission revealed a mass in the retrorectal space. MR scan and anal ultrasound were performed, presenting a fluid-filled cystic mass posterior to the rectum (Fig. 3). Suspecting a congenital cyst at this point, a complete surgical excision of the mass using transanal endoscopic microsurgery was indicated. The histopathological examination of the lesion revealed a tailgut cyst.
Discussion
The first description of a congenital cyst in the literature was presented by Middeldorpf in 1885. Since retrorectal tumors occur rarely a correct diagnosis is often found delayed and this lesion is primarily confused with an inflammatory process. The differential diagnosis of retrorectal masses includes many structures like primary tumors of neurogenic, osteogenic, and congenital origin, as well as metastatic and inflammatory processes. Possible congenital lesions could be chordomas, teratomas, meningoceles, in addition to developmental cysts (dermoid, epidermoid, enteric duplication, and tailgut cysts). Apart from inflammatory lesions, developmental cysts are the most common masses in the retrorectal space (3). Tailgut cysts are almost always placed within the retrorectal space. A literature review by Killingworth and Gandacz showed only very few cases occurring outside the retrorectal space (3). Although tailgut cysts are rare lesions, they are being reported with increasing frequency in the literature.
Like in our three cases tailgut cysts are most commonly seen in adult women (2). However, since pelvic and gynaecologic examinations are most frequent within the reproductive years, the female predominance may be artificial. The majority of patients have a palpable extrarectal mass on digital rectal examination emphasizing the importance of this simple, cost effective method for symptomatic as well as asymptomatic patients. In this context Jao even describes a positive result in up to 97% of the cases if displacing the rectum anteriorly (6). Buchs found an incidence of 75% (2). In the largest reported case series of tailgut cysts (n = 53) Hjermstad and Helwig found approximately half of the patients showing symptoms (1). Perirectal pain in addition to symptoms of mass effect: rectal fullness, bleeding, and change in urinary and stool frequency is the most frequent observation. Although rare, outlet obstruction causing obstipation should alert about the possibility of a mass in the retrorectal space. Furthermore, recurrent abscess-fistula formation in the posterior anal plane should be accompanied by further investigation of the retrorectal space to rule out such kind of masses.
Malignancy arising from a tailgut cyst is rarely reported with a few cases of widespread metastases and death (1). The majority of reported malignancies were adenocarcinomas.
Definitive diagnosis of developmental cyst can be achieved by several diagnostic methods. Due to their location, almost all retrorectal tumors are palpable on rectal examination, and developmental cysts will manifest as extrinsic cystic masses (3). Apart from this straightforward examination a combination of other diagnostic tools can lead to a more accurate differential diagnosis of a retrorectal mass. In our first case a preoperative diagnosis of a developmental cyst was achieved by endoscopy and MRI. In the other third case endorectal ultrasound was added.
While endoscopy can reveal any rectal mucosal changes, endorectal sonography is able to characterize the lesion as cystic. In literature there are limited reports of MRI findings of tailgut cysts. Although MR scans have limited capability to detect calcifications it can diagnose fatty tumours using fat suppression. Sagital films can evaluate structural relationships (3).
The definitive diagnosis and treatment of a tailgut cyst is achieved through complete surgical excision (3). Biopsy should be avoided if possible. In order to prevent recurrence, infection, and a rare but possible malignant transformation a complete excision is necessary. Therefore the surgical approach should be discussed intensely.
As far as we know this is the first report of retrorectal tumours resected by means of transanal endoscopic microsurgery. The well-known benefits of this technique, mostly used for rectal adenoma and well selected T1 carcinomas, could also be applied to this kind of tumours of the retrorectal space (7). By using TEM a more aggressive approach like the Kraske procedure can be avoided. The reason we defend the TEM approach in comparison to other surgical techniques when treating retrorectal tumours, lies in the beneficial combination of an optical system with 3D-view, sixfold magnification and the resolution of the human eye. In combination with the creation of a stable pneumorectum, as well as the use of specially designed instruments, it allows the excision through the rectal wall under excellent view. Furthermore, a more accurate excision enables a proper histological examination and avoids recurrences. This case report should therefore alert surgeons about the benefits of a transanal route using TEM for the excision of retrorectal masses.
References
1. Hjermstad BM, Helwig EB. Tailgut cysts. Report of 53 cases. Am J Clin Pathol 1988, 89: 139-47. [ Links ]
2. Buchs N, Taylor S, Roche B. The posterior approach for low rectal tumors in adults. Int J Colorectal Dis 2007; 22 (4): 381-5. [ Links ]
3. Killingworth C, Gadacz TR. Tailgut cyst (retrorectal cystic hamartoma): Report of a case and review of the literature. Am Surg 2005; 71: 666-73. [ Links ]
4. Krones CJ, Peiper C, Griefingholt H, Schumpelick V. Schwanzdarmzyste-Seltene Differenzialdiagnose retrorektaler Tumoren. Chirurg 2002; 73: 1123-6. [ Links ]
5. Gönül II, Baglan T, Pala I. Tailgut cyst: diagnostic challenge for both pathologists and clinicians. Int J Colorectal Dis 2006; May 16 -DOI 10.1007/s00384-006-0153-2. [ Links ]
6. Jao SW, Beart RW Jr, Spencer RJ. Retrorectal tumors: Mayor Clinic Experience, 1960-1979. Dis Colon Rectum 1985; 28: 644-52. [ Links ]
7. Palma P, Freudenberg S, Samel S, Post S. Transanal endoscopic microsurgery: Indications and results after 100 cases. Colorectal Dis 2004; 6: 350-5. [ Links ]
![]() Correspondence:
Correspondence:
Pablo Palma.
Sección de Coloproctología.
Servicio de Cirugía General y Aparato Digestivo.
Hospital Universitario "Virgen de las Nieves".
18012 Granada.
e-mail: pablopalma@andaluciajunta.es
Recibido: 30-03-07.
Aceptado: 11-04-07.

