










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.101 n.3 Madrid Mar. 2009
PICTURES IN DIGESTIVE PATHOLOGY
Perianal leiomyoma
Leiomioma perianala
S. Salvans Ruiz, J. Gimeno Beltrán1 and D. Parés
Unit of Colorectal Surgery. Departments of General Surgery and 1Pathology. Hospital del Mar. Barcelona, Spain
Case report
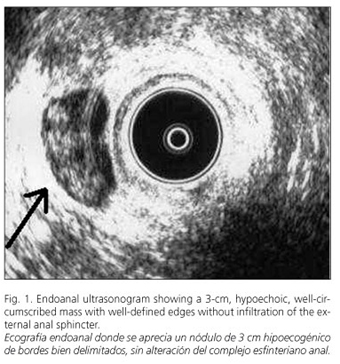
A 74-year-old female was admitted to our hospital with a one-year history of perianal tumor that required antibiotic treatment on several occasions for infection. Physical examination revealed a clearly painful, soft, smooth nodule with well-delimited edges located in the right anterior quadrant of the anal canal. The remaining physical exam did not reveal any significant abnormality. An endoanal ultrasound (EUS) was performed which detected a 3-cm hypoechoic, well-circumscribed nodule without infiltration of the external anal sphincter (Fig. 1). Abdomino-pelvic T1-weighted magnetic resonance imaging (MRI) confirmed this well-defined lesion in the same site without contact with the internal and external anal sphincters (Fig. 2). Surgical treatment was indicated and a well-defined 3-cm mass without contact with the anal sphincter was discovered and excised.

The final histopathological diagnosis was vascular leiomyoma (Fig. 3).

Discussion
Vascular leiomyoma is a benign tumor derived from mesenchymal cells (1). Its clinical presentation in the gastrointestinal tract is very uncommon, and it more usually affects the skin and genital tract in women (2). While the stomach and small intestine are the most frequently involved areas, the colon and rectum are less likely sites (2,3). The anorectal region includes less than 0.1% of all rectal tumors (4,5). Despite its ability to present at any age without gender distinctions, its higher frequency occurs in middle-aged females (3-5). The typical clinical presentation is a palpable mass next to the anus. However bleeding and constipation may also occur (3,5). EUS is the first test that allows, as does MRI, to assess the characteristics of this lesion and its relationship with the anal sphincters (4). A definitive diagnosis is reached by histopathology, and therefore the first therapeutic option is surgical excision (3,4).
References
1. Wiech T, Walch A, Werner M. Histopathological classification of nonneoplastic and neoplastic gastrointestinal submucosal lesions. Endoscopy 2005; 37: 630-4. [ Links ]
2. Gómez NA, Cozzarelli R, Álvarez LR, Fabre E, Vargas PE, Zapatier JA. Rectum leiomyoma in a 10-month-old female. Pediatr Surg Int 2003; 19: 104-5. [ Links ]
3. Sasaki K, Gotoh Y, Nakayama Y, Hayasaka H, Ishiyama Y, Miyashita H. Leiomyoma of the rectum. Int Surg 1985; 70: 149-52. [ Links ]
4. Bracey EECL, Mathur P, Dooldeniya M, Joshp A, Dawson PM. Unusual perianal tumours masquerading as abscesses. Int J Clin Pract 2003; 57: 343-6. [ Links ]
5. Hatch KF, Blanchard DK, Hatch GF 3rd, Wertheimer-Hatch L, Davis GB, Foster RS Jr, et al. Tumors of the rectum and anal canal. World J Surg 2000; 24: 437-43. [ Links ]

