










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.101 no.4 Madrid abr. 2009
Natural orifice transluminal endoscopic surgery (NOTES)
Cirugía endoscópica transluminal por orificios naturales (NOTES)
M. J. Varas Lorenzo, J. C. Espinós Pérez1 and M. Bardají Bofill2
Units of Echoendoscopy, 1Endoscopy and 1Digestive Surgery. Centro Médico Teknon. Barcelona, Spain
ABSTRACT
A current review and update of an exceedingly novel and appealing topic, namely natural orifice transluminal endoscopic surgery (NOTES), is discussed, as well as the authors' viewpoint thereon. Most reviewed studies were performed in laboratory animals, but reports on transvaginal cholecystectomy and the emergence of editorials and review articles on this topic pose a number of as yet unanswered questions on this type of surgery, which represents a potential advance towards "endoscopic surgery with no scars, no infection, minimal anesthesia requirements, and immediate recovery".
Key words: NOTES. Natural orifice transluminal endoscopic surgery. Laparoscopic surgery.
RESUMEN
Se presenta una revisión actual, puesta al día, y punto de vista de los autores sobre un tema sumamente novedoso y atractivo, como es la Cirugía Endoscópica Transluminal por Orificios Naturales (NOTES: Natural Orifice Translumenal Endoscopic Surgery). La mayoría de los trabajos revisados se han realizado en animales de experimentación, pero la publicación de la colecistectomía por vía transvaginal, y la aparición de editoriales y artículos de revisión sobre el tema, nos llevan a realizar una serie de preguntas no resueltas actualmente sobre este tipo de cirugía, que representa un avance potencial para conseguir “una cirugía endoscópica sin cicatrices, sin infecciones, con mínimos requerimientos de anestesia y una inmediata recuperación”.
Palabras clave: NOTES. Cirugía endoscópica transluminal por orificios naturales. Cirugía laparoscópica.
Introduction
Conventional surgery using laparotomy has been greatly replaced by laparoscopic surgery; classical incisions have been substituted for by "small incisions or orifices" through which trocars and laparoscopes are introduced, which has revolutionized abdominal and digestive surgery. Laparoscopic cholecystectomy has already become a classic approach, and is even performed under sonographic guidance (USLap).
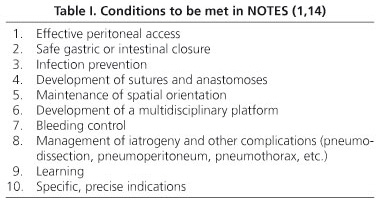
Based on minimally invasive surgery, a novel approach to endoluminal endoscopic surgery is currently emerging that takes advantage of natural orifices (NOTES), aimed at eliminating scars and scar-related complications (pain, herniation, infection) in the abdomen (a more esthetic surgery), and promoted by the NOSCAR team (1) (Table I).
Minimally invasive surgery
Three radically novel concepts were applied to surgery 20 years ago - that incision size "does matter", as it influences postoperative course and outcome (paralytic ileus); that surgery must be a multidisciplinary activity; and that technology is essential for surgeons in the development of laparoscopic surgery versus minilaparotomy. These three concepts apply to NOTES.
Endoscopic digestive surgery
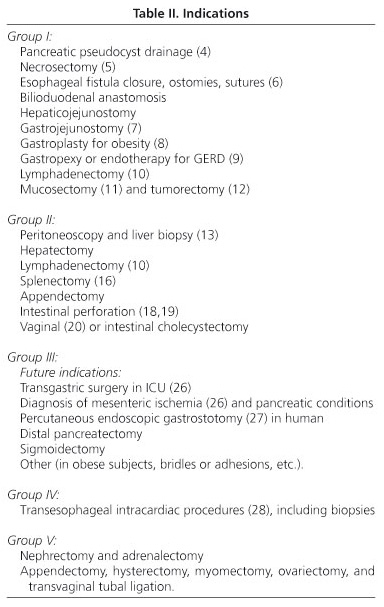
ERCP-mediated sphincterotomy, pancreatic pseudocyst drainage (2-10), mucosectomy (11) or endoscopic mucosal resection (EMR), endoscopic submucosal dissection (ESD), endoscopic muscular dissection (EMD), tumorectomy (12), and transanal endoscopic microsurgery (TEM) have been carried out via an endoscope introduced into the body through the mouth or anus, also aided by or under the guidance of endoscopic ultrasounds (EUS) (Table II).
Transluminal endoscopic surgery (NOTES)
Transluminal access may be gained via the transesophageal, transgastric, transesophago-gastro-duodenal (transoral), transcolonic, transvaginal, and transvesical routes using multichannel endoscopes and prototypes - Karl Storz, dual-channel Olympus-R, curved, four-channel Transport & Cobra, Pentax, Wolf.
Flexible peritoneoscopy and liver biopsy are mainly performed via the transgastric route (13), but the term "transluminal" implies a direct entry of the endoscope into the peritoneal cavity through natural internal orifices in the stomach, colon or vagina (14).
Natural external and internal orifices
An endoscope may be introduced through a natural external orifice such as the mouth, anus, vagina, and urethra to visualize various cavities and to use incisions and sutures (6) to create internal orifices for entry into the free peritoneal cavity and access to different viscera (Table III), including the gallbladder (15), spleen (16), liver, and female genitalia (17), for surgery. Intestinal and gastric perforations could also be closed (18,19).
These procedures are most often performed via the transgastric, transcolonic, and transvaginal routes, and the first transvaginal cholecystectomy in humans (Operation ANUBIS) (20) has already been carried out. Also, the first transgastric appendectomies in humans (unpublished) were performed by Rao and Reddy in India in 2004.
A transvesical route has been recently implemented (21), and experimental work is now being conducted regarding a combined transgastric-transvesical route (22), or a hybrid transgastric-laparoscopic approach for cholecystectomy.
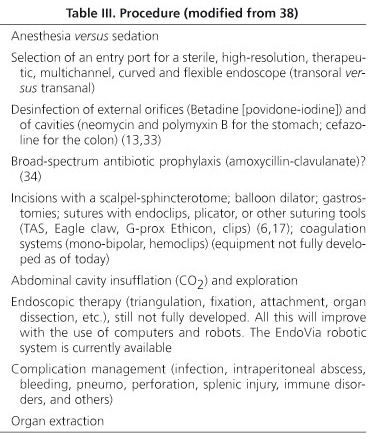
Materials used in notes
Pneumoperitoneum will be performed using a Veres needle at the bottom of the navel, with trocars, laparoscopes or minilaparoscopes (3-mm trocars) for hybrid techniques.
However, true NOTES will use special 120 mm-long, high-resolution flexible videoendoscopes with multiple channels to reach the abdominal cavity. As discussed above, a number of different manufacturers exist. Overtubes will be used. The Shape Lock technology, a shared platform and support for videoendoscopes, is now available. A robotic EndoVia device is also available that may help in therapeutic endoscopy.

Opening equipment will include scalpels, papillotomes, laser, polyethylene balloon dilators, etc., as well as resection and closure (suture) materials (Eagle Claw) (Plicator) (Esophyx-Palex), anastomosis materials, etc.
Suture and anastomosis materials for the stomach and colon are very important in view of perforation and peritonitis risks.
Dissection and vascular coagulation materials will also be used (monopolar, bipolar, bipolar/multipolar electrocoagulation; clips, etc.), as well as 20- or 30-mm Endoloop, and a plastic bag for resected organs (Unimax) with mouse-tooth forceps (43).
All this equipment is not fully developed as of today. NOTES-specific materials will be available in the future.
Aids in the form of endoscopic ultrasounds (EUS) and miniprobes (MPs) will be used on occasion, probably not often. Radial or sectorial Doppler echoendoscopes, currently 5 to 20-MHz electronic devices, will be used to facilitate the study of vessels, or even 12- or 15-MHz miniprobes, with balloons to provide good acoustic windows; thus, the risk for potential complications would be reduced (Table II).
Discussion
From recent reviews (23-26,37-42) and studies, primarily in research animals, the following considerations ensue:
-Transesophageal route. This route will likely be used for transesophageal intracardiac procedures (group IV), including biopsies, aided by or under guidance of EUS (28). Radial and sectorial EUS with FNAP will be essential for transesophageal route procedures.
-Transgastric route. Group-I indications are already being carried out through the transgastric or transduodenal route under EUS. A clear instance is pseudocyst and abscess drainage, and EUS-guided pancreatic necrosectomies, which represent a "notable" advance for NOTES.
Indications in groups II and III represent the true targets for NOTES: lymphadenectomy, cholecystectomy, splenectomy, appendectomy, pancreatectomy, sigmoidectomy, and other procedures such as ventral hernia repair (29). Of these, only distal pancreatectomy will probably require EUS support along the stomach's greater curvature to locate an entry point for distal pancreatic resection. Miniprobes (MPs) may also likely help in selecting an entry point.
-Transcolonic route. Besides TEM (30-31) for uT0-uT1N0 tumors, submucosal tumors, and retrorectal cysts (32), this route will allow the closure of intestinal perforations and drainage of fluid collections, as well as cholecystectomies (33) and appendectomies via the trans-sigmoidal route (34), always under ERUS (endorectal ultrasounds) or EUS.
-Transvaginal route. Numerous procedures have already been performed through this route, some of them indicated in group V. Most novel among these is transvaginal cholecystectomy (20).
NOTES represents a new field that is drawing the attention of surgeons and endoscopists alike. Potential future applications cannot be established yet, nor can potential benefits regarding the development of new complications (opening of hollow viscera with peritonitis risk, failed sutures, etc.) be ascertained.
Research with animals must continue for visceral disinfection techniques, optimal entry points for each organ and procedure, potential need of EUS or MPs, optimal approach (scalpel, puncture, dilation), insufflation mode, sustained sterility for endoscopes, need for one versus several access points, and closure of openings for organ access; most relevantly, new technology is needed to provide materials equivalent to those of laparoscopy but usable through flexible endoscopes 120 cm in length, and with several work channels 3.5-4.2 mm in diameter.
The precise usefulness and real indications of NOTES will be established once these questions are answered and material advances have taken place, when its complications versus benefits ratio is seen to be superior to that provided by other techniques such as laparoscopy.
Another debated topic is who should perform this technique and where. Surgeons reconverted to endoscopy? Surgeons assisted by endoscopists? Endoscopists supported by surgeons? In the operating room? In the endoscopy room? Should patients be sedated or anesthesized? Surely, some indications will be carried out by gastroenterologists-endoscopists with no surgical training but expertise in therapeutical endoscopy, whereas other indications involving visceral resection and risk of surgical conversion should be taken in charge by surgeons with endoscopic training. The booming of this novel technique may perhaps lead to changes in specialty/subspecialty fields and education, with the emergence of "endoscopist surgeons". Or maybe nothing will come of this, as was the case with biliary lithotripsy or more recently with anti-reflux management.
Both at present and in the future, cholecystectomy and probably appendectomy represent the primary surgical targets, and will be performed using the transgastric (36), transvaginal (20), or trans-sigmoidal route, maybe a combined (transgastric-transvaginal, transgastrica-transvesical) route, or even the transumbilical route, but many, highly appealing indications exist (44-51) that account for the interest in this approach, and awake optimism regarding the achievement of intended goals: "Surgery with no scars or infection, minimal anesthesia requirements, and immediate recovery".
¿What are the indications, benefits and drawbacks or laparoscopic or minilaparoscopic cholecystectomy, and of NOTES cholecystectomy?
¿Will NOTES cholecystectomy be cost-effective? (Table IV).
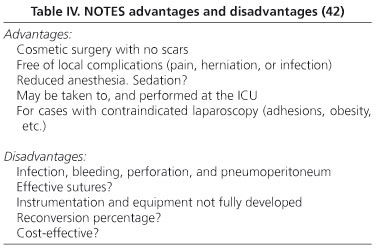
We do believe in multidisciplinary teams, that technological advances will provide materials specific for this type of surgery, and that the true indications of NOTES will eventually be established.
![]() Correspondence:
Correspondence:
Modesto José Varas Lorenzo.
Unidad de Ecoendoscopia.
Centro Médico Teknon.
C/ Marquesa de Vilallonga, 12.
08017 Barcelona, Spain.
email: varas@dr.teknon.es
Received: 01-12-08.
Accepted: 15-01-09.
References
1. Rattner D, Kalloo A. ASGE/ SAGES Working Group. ASGE/SAGES Working Group on Natural Orifice Translumenal Endoscopic Surgery. October 2005. Surg Endosc 2006; 20: 329-33. [ Links ]
2. Rocca R, De Angelis G, Castellino F, et al. EUS diagnosis and simultaneous endoscopic retrograde cholangiography treatment of common bile duct by using an oblique-viewing echoendoscope. Gastrointest Endos 2006; 63: 479-84. [ Links ]
3. Bories E, Caillol F, Pesenti C, Giovannini M. Safety and efficacy of a diagnostic strategy combining therapeutic endoscopic retrograde endoscopy and endosonography during the same anaesthesiology. Retrospective study about 98 patients. Endoscopy 2007; 39 (Supl. 1): A377. [ Links ]
4. Kahaleh M, Shami VM, Conoway MR, et al. Endoscopic ultrasound drainage of pancreatic pseudocyst: a prospective comparison with conventional endoscopic drainage. Endoscopy 2006; 38: 355-9. [ Links ]
5. Seewald S, Groth S, Omar S, et al. Aggressive endoscopic therapy for pancreatic necrosis and pancreatic abscess: a new safe and effective treatment algorithm. Gastrointest Endosc 2005; 62: 92-100. [ Links ]
6. Fritscher-Ravens A. EUS-guided endosurgery. In: Dietrich ChF, editor. Endoscopic Ultrasound. Stuttgart: Thieme; 2006. p. 378-86. [ Links ]
7. Fritscher-Ravens A, Mosse CA, Mukherjee D, et al. Transluminal endosurgery: single lumen access anastomotic device for flexible endoscopy. Gastrointest Endosc 2003; 58: 585-91. [ Links ]
8. Hu B, Chung SCS, Sun LCL, et al. Transoral obesity surgery: endoluminal gastroplasty with an endoscopic suture device. Endoscopy 2005; 37: 411-4. [ Links ]
9. Fritscher-Ravens A, Mosse CA, Mukherjee D, et al. Transgastric gastropexy and hiatal hernia repair for GERD under EUS control: a porcine model. Gastrointest Endosc 2004; 59: 89-95. [ Links ]
10. Fritscher-Ravens A, Mosse CA, Ikeda K, et al. Endoscopic transgastric lymphadenectomy by using EUS for selection and guidance. Gastrointest Endosc 2006; 63: 302-6. [ Links ]
11. Miquel JM, Abad R, Souto J, et al. EUS-guided mucosectomy for gastrointestinal cancer. Rev Esp Enferm Dig 2006; 98: 591-6. [ Links ]
12. Martínez-Ares D, Varas MJ, Souto J, et al. Endoscopic resection gastrointestinal submucosal tumors asisted by endoscopic ultrasonography. Surg Endoscopic 2005; 19: 854-8. [ Links ]
13. Kalloo AN, Singh VK, Jagannath SB, et al. Flexible transgastric peritoneoscopy: A novel approach to diagnostic and therapeutic interventions in the peritoneal cavity. Gastrointest Endosc 2004; 60: 114-7. [ Links ]
14. Bowman DE. ASGE/SAGES Working Group on natural orifice transluminal endoscopic surgery: White Paper October 2005. Gastrointest Endosc 2006; 63: 199-203. [ Links ]
15. Park PO, Bergstrom M, Ikeda K, et al. Experimental studies of transgastric gallbladder surgery: cholecystectomy and cholecystogastric anastomosis. Gastrointest Endosc 2005; 61: 601-6. [ Links ]
16. Kantsevoy SV, Hu B, Jagannnath SB, et al. Transgastric endoscopic splenectomy: is it possible? Surg Endosc 2006; 20: 522-5. [ Links ]
17. Fritscher-Raven A. Transgastric endoscopy - a new fashion, a new excitement! Endoscopy 2007; 39: 161-7. [ Links ]
18. Raju GS, Shibukawa G, Ahmed I, et al. Endoluminal suturing may overcome the limitations of clip closure of a gaping wide colon perforation (with videos). Gastrointest Endosc 2007; 65(6): 906-11. [ Links ]
19. Park P, Raju G, Swain P, et al. Randomized multicenter controlled study of endoscopic and surgical closure of a gastric NOTES access perforation in a porcine model. Endoscopy 2007; 39(Supl. 1): A61. [ Links ]
20. Marescaux J, Dallemagne B, Perretta S, et al. Report of transluminal cholecystectomy in a human being. Arch Surg 2007; 142: 823-6. [ Links ]
21. Gettman MT, Blute ML. Transvesical peritoneoscopy: initial clinical evaluation of the bladder as a portal for NOTES. Mayo Clin Proc 2007; 82: 843-5. [ Links ]
22. Rolanda C, Lima E, Pego JM, et al. Third-generation cholecystectomy by natural orifices: transgastric and transvesical combined approach. Gastrointest Endosc 2007; 65: 111-7. [ Links ]
23. Giday SA, Kantsevoy SV, Kalloo AN. Principle and history of natural orificie translumenal endoscopic surgery (NOTES). Minim Invasive Ther Allied Technol 2006; 15: 373-7. [ Links ]
24. Baron TH. NOTES. Br J Surg 2007; 94: 1-2. [ Links ]
25. Willingham FF, Brugge WR. Taking NOTES: translumenal flexible endoscopy and endoscopy surgery. Current Opinion in Gastroenterol 2007; 23: 550-5. [ Links ]
26. Pearl JP, Ponsky JL. NOTES: past, present and future. J Min Access Surg 2007; 3: 43-6. [ Links ]
27. Marks JM, Ponsky JL, Pearl JP, et al. PEG "Rescue": A practical NOTES technique. Surg Endosc 2007; 21: 816-9. [ Links ]
28. Fritscher-Ravens A, Ganbari A, Mosse CA, et al. Transesophageal endoscopic ultrasound-guided access to the heart. Endoscopy 2007; 39: 385-9. [ Links ]
29. Hu B, Kalloo AN, Chung SSC, et al. Peroral transgastric endoscopic primary repair of a ventral hernia in a porcine model. Endoscopy 2007; 39: 390-3. [ Links ]
30. Swanström LL. Transanal endoscopic microsurgery: current indications and techniques. J Gastrointest Surg 2000; 4: 342-3. [ Links ]
31. Palma P, Freudenberg S, Samel S, et al. Transanal endoscopic microsurgery: indications and results after 100 cases. Colorectal Dis 2004; 6: 350-5. [ Links ]
32. Zoller S, Joos A, Dinter D, et al. Retrorectal tumors: excision by transanal endoscopic microsurgery. Rev Esp Enferm Dig 2007; 99: 547-50. [ Links ]
33. Pai RD, Fong DG Bundga ME, et al. Transcolonic endoscopic cholecystectomy: a NOTES survival study in a porcine model. Gastrointest Endosc 2006; 64: 428-34. [ Links ]
34. Wilhelm D, Meining A, von Delius S, et al. An innovate, safe and sterile sigmoid access (ISSA) for NOTES. Endoscopy 2007; 39: 401-6. [ Links ]
35. Whiterford MH, Denk PM, Swanström LL. Feasibility of radical sigmoid colectomy performed as natural orifice translumenal endoscopic surgery (NOTES) using transanal endoscopic microsurgery. Surg Endoscopy 2007; 21: 1870-4. [ Links ]
36. Sumiyama K, Gostout CJ, Rajan E, et al. Transgastric cholecystectomy: transgastric accessibility to the gallbladder improved with the SEMF meted and a novel multibending therapeutic endoscope. Gastrointest Endosc 2007; 65: 1028-34. [ Links ]
37. Vitale GC, Davis BR, Tran TC. The advancing art and science of endoscopy. Am J Surg 2005; 190: 228-33. [ Links ]
38. Swanström LL. Desarrollo tecnológico actual de la cirugía endoscópica transluminal a través de orificios naturales. Cir Esp 2006; 80: 283-8. [ Links ]
39. Wagh MS, Thompson CC. Surgery insight: natural orifice transluminal endoscopic surgery -an analysis of work to date. Nat Clin Pract Gastroenterol Hepatol 2007; 4: 386-92. [ Links ]
40. Babatin A. NOTES: envolving trends in endoscopic surgery. Saudi J Gastroenterol 2007; 13: 207-10. [ Links ]
41. Swain P. A justification for NOTES -natural orificie transluminal endosurgery. Gastrointest Endosc 2007; 65: 514-6. [ Links ]
42. Varas MJ, Espinós JC, Abad R, et al. Endocirugía asistida por Endosonografía (USE). En: Varas MJ, editor. Ultrasonografía endoscópica. Madrid, Panamericana; 2008. p. 313-20. [ Links ]
43. Dolz C, Noguera JF, Martín A, et al. Colecistectomía transvaginal (NOTES) combinada con minilaparoscopia. Rev Esp Enferm Dig 2007; 99: 698-702. [ Links ]
44. Noguera JF, Dolz C, Cuadrado A, et al. Transvaginal liver resection (NOTES) combined with minilaparoscopy. Rev Esp Enferm Dig 2008; 100 (7): 411-5. [ Links ]
45. Zornig C, Mofid H, Emmermann A, et al. Scarless cholecystectomy with combined transvaginal and transumbilical approach in a series of 20 patients. Surg Endosc 2008; 22 (6): 1427-9. [ Links ]
46. Ramos AC, Murakami A, Galvao Neto M, et al. Notes transvaginal video-assisted cholecystectomy: firts series. Edoscopy 2008; 40(7): 572-5. [ Links ]
47. Palanivelu C, Rajan PS, Rangarajan M, et al. Transvaginal endoscopic appendectomy in humans: a unique approach to notes-world's first report. Surg Endosc 2008; 22(5): 1343-7. [ Links ]
48. Zhu JF, Hu H, Ma YZ, Xu MZ, Li F. Transumbilical endoscopic surgery: a preliminary clinical report. Surg Endosc 2009; 23(4): 813-7. [ Links ]
49. Lacy AM, Delgado S, Rojas OA, et al. MA-NOS radical sigmoidectomy: report of a transvaginal resection in the human. Surg Endosc 2008; 22 (7): 1717-23. [ Links ]
50. Sylla P, Willingham FF, Sohn DK, et al. NOTES rectosigmoid resection using transanal endoscopic microsurgery (TEM) with transgastric endoscopic assistence: a pilot study in swine. J Gastrointest Surg 2008; 12(10): 1717-23. [ Links ]
51. Swain P. Nephrectomy and NOTES: transvaginal, transgastric, transrectal, and transvesical approaches. J Endourol 2008; 22(4): 811-8. [ Links ]
52. Flora E, Wilson T, Martin I, et al. A review of natural orifice translumenal endoscopic surgery (notes) for intra-abdominal surgery: experimental models, techniques, and applicability to the clinical setting. Annals Surg 2008; 247: 583-602. [ Links ]
53. Hookey LC, Khokhotva V, Bielawska B, et al. The Queen's closure: a novel technique for closure of endoscopic gastrostomy for natural-office transluminal endoscopic surgery. Endoscopy 2009; 41: 149-53. [ Links ]
54. Cugat E, Varas MJ. Cirugía endoscópica por orificios naturales (NOTES), ¿Visión de futuro? Rev Esp Enferm Dig 2008; 100(7): 383-6. [ Links ]
55. Swanström LL. Natural orifice transluminal endoscopic surgery. Endoscopy 2009; 41: 82-5. [ Links ]

