










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.101 no.9 Madrid sep. 2009
Endoscopic ultrasound in the diagnosis and staging of pancreatic cancer
J. Iglesias García, J. Lariño Noia and J. E. Domínguez Muñoz
Gastroenterology Department. Foundation for Research in Digestive Diseases. University Hospital of Santiago de Compostela. A Coruña, Spain
ABSTRACT
Pancreatic cancer is the 5th leading cause of cancer-related death in Western countries. The 5-year survival rate is approximately 4%, without significant changes over the last 50 years. This poor survival rate and bad prognosis are associated with the diagnosis of advanced-stage disease, which precludes the only potential curative treatment - surgical resection. In this setting, the main objective in the management of pancreatic cancer is to perform an early diagnosis and a correct staging of the disease. Endoscopic ultrasonography (EUS) appears to be an essential tool for the diagnosis and staging of pancreatic cancer. EUS diagnostic accuracy for detecting pancreatic tumors ranges from 85 to 100%, clearly superior to other imaging techniques. EUS accuracy for the local staging of pancreatic cancer ranges from 70 to 90%, superior or equivalent to other imaging modalities. EUS-guided fine-needle aspiration allows a cyto-histological diagnosis in nearly 90% of cases, with a very low complication rate. At present, the formal indications for EUS-guided fine-needle aspiration are the necessity of palliative treatment or whenever the possibility of neoadjuvant treatment is present. It could be also indicated to differentiate pancreatic adenocarcinoma from other pancreatic conditions, like lymphoma, metastasis, autoimmune pancreatitis or chronic pancreatitis. We can conclude that EUS is an essential tool in the management of patients with pancreatic tumors.
Key words: Endoscopic ultrasound. Pancreatic cancer. Diagnosis. Stanging.
Introduction
Pancreatic cancer is the 5th leading cause of cancer death in Western countries, and the second cause of cancer death among gastrointestinal tumors (1). The 5-year survival rate is approximately 4%, without significant changes over the last 50 years (2). The only group of patients with pancreatic cancer and an acceptable prognosis are those with potentially resectable pancreatic tumors (3).
Bad prognosis in these patients is related to tumor stage, which may preclude the only potentially curable treatment - surgical resection. Traditionally, patients with pancreatic cancer without distant disease underwent a surgical procedure. However, without an adequate preoperative study, the resectabily rate was between 5 and 25%, with high morbidity (3). On the other hand, by performing a correct study prior to surgery, this resectability rate can reach 75% (4). That is the reason why the primary objective in the management of this disease is to perform both an early diagnosis and a correct staging, which will allow to perform the only potentially curative treatment - surgical resection.
Nowadays, there are many procedures to perform the diagnosis and staging of pancreatic cancer. Some of them are abdominal ultrasounds (AU), helical CT, magnetic resonance imaging (MRI), endoscopic retrograde cholangiopancreatography (ERCP), abdominal arteriography, and more recently endoscopic ultrasonography (EUS).
EUS allows a detailed analysis of the pancreatic parenchyma, pancreatic ducts, and all structures adjacent to the pancreas. It has become an essential tool for the study of pancreatic diseases, and is considered the reference method for the diagnosis and staging of inflammatory pancreatic diseases and solid pancreatic tumors, as well as a key point in the diagnostic and staging algorithms for pancreatic tumors (5,6).
The aim of this article is to perform an exhaustive revision of the literature regarding the usefulness of EUS in the diagnosis and staging of pancreatic cancer. First we will analyze its usefulness in the diagnosis of pancreatic tumors, afterwards we will discuss its accuracy in the evaluation of local infiltration and lymph-node extension. Finally we will focus on the importance of cyto-histological evaluation for pancreatic tumors.
Endoscopic ultrasounds in the diagnosis of pancreatic tumors
When analyzing the results of the most important and best-designed studies, the sensitivity of EUS for the diagnosis of solid pancreatic tumors was 96% (range 85-100%) (7-27). However, these studies included benign pancreatic diseases and ampullary tumors, and this may bias the analysis in favor of EUS (7-10,16,17,22-24). But if we only evaluate studies regarding malignant pancreatic tumors, the diagnostic sensitivity is still very high, clearly superior to that of other imaging techniques. When EUS was compared to conventional CT (8,9,11-17,21-24,26,27), EUS diagnostic sensitivity was superior (98 vs. 77%, p < 0.0001), and differences remained when the comparison was performed with helical CT (16,18,22-24). Among all these studies, we should focus in two of them comparing EUS and multidetector-row CT. In a retrospective study published by Agarwal et al. (26), including 81 patients, EUS sensitivity for tumor detection was 94%, while CT only reached 86%. DeWitt et al. (27) published similar data. They performed a comparative, prospective, cohort study, including 120 patients. EUS sensitivity for tumor detection (98%) was superior to that of multidetector-row CT (86%).
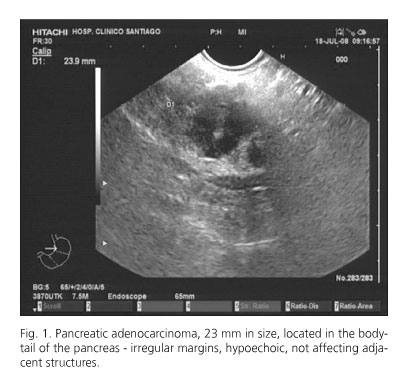
But the point in which EUS has demonstrated to be clearly more accurate is in the identification of small pancreatic tumors (Fig. 1), which have been undetected by other imaging techniques (7,8,12,18,22,26,27-29). For tumors between 15 and 35 mm, Legman et al. (18) reported that EUS and helical CT both detected all tumors in 14 patients; however, when analyzing tumors smaller than 15 mm, EUS detected 6 of 6 cases, whereas CT could only detect 4. Muller et al. (12) analyzed the sensitivity of EUS, CT and MRI in the identification of tumors smaller than 3 cm, showing values of 93, 53 and 67%, respectively. In the same article, for tumors smaller than 2 cm, the sensitivity of each was 90, 40 and 33%, respectively. Ardengh et al. (28) performed a retrospective study including 17 patients with tumors smaller than 3 cm. EUS identified the pancreatic tumor in all cases (100%), whereas CT could only identify the tumor in 94% of cases. However, only the study by DeWitt et al. (27) was performed with multidetector-row CT in this group of patients with smaller tumors. In their study, including 19 patients with tumors smaller than 25 mm, they reported a non-significant trend towards improved detection by EUS as compared to multidetector-row CT (89 vs. 53%, p = 0.08). Recently, two new papers have confirmed these data, showing that EUS allows to detect pancreatic lesions not clearly visualized by CT or MRI, and is able to diagnose pancreatic tumors (from pancreatic adenocarcinomas to pancreatic metastases or endocrine tumors) in nearly 65% of cases (30,31).
EUS is also considered very accurate in ruling out the presence of a pancreatic tumor. Catanzaro et al. (32) retrospectively identified 80 patients with clinical suspicion of pancreatic cancer and normal EUS. After a mean follow-up of 24 months, one patient with evidence of chronic pancreatitis on EUS was found to have a pancreatic cancer at surgery. No patient with normal pancreatic EUS results developed cancer during the follow-up period. In the study performed by Agarwal et al. (26) in patients with clinical suspicion of pancreatic cancer, and without identifiable lesions on multidetector-row CT, the diagnostic accuracy of EUS was 92%, able to exclude the presence of a pancreatic tumor when EUS was normal.
In this context, the most important paper summarizing all the above data has been the systematic review published by DeWitt et al. (33). They compared CT and EUS for the diagnosis of pancreatic cancer. They analyzed the 11 better-designed studies, including a total of 678 patients. Nine of these studies analyzed the diagnostic accuracy of EUS for the detection of pancreatic tumors. All studies included were consecutive series of patients, with a good standardization of imaging techniques, independently compared to the gold standard, and almost all were prospective studies. In all these studies, the diagnostic sensitivity of EUS was superior to that of helical CT, even more so for pancreatic tumors smaller than 3 cm. They concluded that EUS is superior to CT for the detection of pancreatic cancer.
Endoscopic ultrasounds in the staging of pancreatic cancer
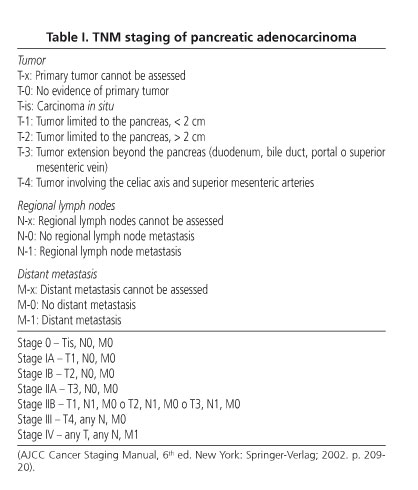
At this point we will review the existing evidence on local staging (with specific data on vascular and lymph-node infiltration) and the evaluation of resectability. The staging of pancreatic cancer is based on the TNM classification published by AJCC in 2002 for pancreatic adenocarcinoma (Table I).
Local staging
Several studies have been published evaluating the accuracy of EUS in the loco-regional staging of pancreatic cancer, in most cases compared to CT scanning, and in more recent studies with MRI and/or selective abdominal arteriography. Globally, the reported accuracies of local staging by EUS in pancreatic cancer range from 62 to 94%, and those of nodal staging range from 72 to 92% (34-46). The most important study, as previously mentioned, has been the systematic review published by DeWitt et al. (33), comparing CT and EUS for the staging of pancreatic cancer. In this setting, the authors analyzed the 11 best designed studies, including a total of 678 patients, comparing the accuracy of both techniques for the local staging of this tumor. All studies included were consecutive series of patients with a good standardization of imaging techniques, independently compared to the gold standard, and almost all were prospective studies. The authors conclude that EUS appears to be superior to CT for T-staging and regarding the vascular invasion of the splenoportal confluence; however both techniques appear to be equivalent for nodal staging and overall vascular invasion.
Vascular invasion
For the overall evaluation of vascular invasion the accuracy of EUS ranges from 40 to 100% (14,15,21,23, 24,38,41,42). The sensitivity and specificity of EUS for malignant vascular invasion range from 42 to 91% and from 89 to 100%, respectively (21,38,41,42,47). However, when comparing EUS to CT in this setting, some studies have demonstrated that EUS is more accurate (14,21,23,24), and other authors have reported that the accuracy of CT is superior (15,41,42). MRI showed similar results to EUS (41,42). When evaluating the different vessels separately, for venous invasion EUS demonstrated to be equal or superior to CT, with a sensitivity and overall accuracy of 56 and 50%, respectively (11,13). For the evaluation of portal vein and confluence invasion, the sensitivity of EUS increases to 60-100%, in all cases superior to all other imaging techniques (7,9,17,22,48). However, for the evaluation of the superior mesenteric vein, superior mesenteric artery and celiac axis, the sensitivity of EUS decreases to 17-83% (37), 17% (23) and 50% (9), respectively, with better results for helical CT (9,22,23). This is in contrast to the splenic artery and vein, an area easily seen and staged by EUS (7,48,49). A systematic review of the literature and a meta-analysis have been recently published, analyzing the usefulness of EUS in this setting. A total of 29 studies were evaluated (n = 1,308), in which EUS showed a sensitivity for the detection of vascular invasion of 73%, with a specificity of 90.2% (50).
Lymph node infiltration
The main node stations to be evaluated in pancreatic cancer are the perigastric, periduodenal, and celiac nodes, as well as the hepatic hilium. Mediastinal lymph nodes should also be evaluated (up to 5% of patients with pancreatic cancer may present with lymph node metastases at this level). The accuracy of EUS for N staging ranges from 64 to 82% (9,11,12,19,21,22,24, 27,33-39). Although EUS is highly sensitive for detecting regional lymph nodes, it has difficulties in distinguishing between malignant and inflammatory adenopathies, the performance of a EUS-guided fine-needle aspiration (FNA) of lymph nodes being necessary on many occasions (51-53).
Evaluation of respectability
At present, tumors considered irresectable are those with metastatic disease, invasion of the superior mesenteric artery, celiac axis and hepatic artery, and/or significant invasion of the portal vein and superior mesenteric vein (Fig.2).

In the various series published in the literature, the sensitivity and specificity of EUS for the evaluation of resectability in pancreatic cancer was 69 and 82%, respectively (16,18,21,27,36,39,40,45,54). When comparing EUS to other imaging techniques, results are contradictory. Generally, most studies showed a similar accuracy of EUS, helical CT, and MRI in the evaluation of resectability for pancreatic cancer. The study from Soriano et al should be emphasized (41). The authors found the initial use of CT or EUS more accurate, followed by other technique to complete the evaluation. Tierney et al. (47) suggested that helical CT should be performed initially, and that EUS should also be employed in most patients because of its improved detection of vascular invasion. DeWitt et al. (27) showed similar conclusions, supporting the use of various imaging techniques, mainly EUS and helical CT. Again, the most important study in this setting has been the systematic review published by DeWitt et al. (33) comparing CT and EUS for the evaluation of resectability in pancreatic cancer. In this setting, the authors analyzed 4 out of the 11 best-designed studies, which specifically analyzed this item. All studies included were consecutive series of patients with a good standardization of imaging techniques, independently compared to the gold standard, and almost all were prospective studies. The authors conclude that EUS appears to be superior to CT for the evaluation of resectability in pancreatic cancer.
EUS can also help in the evaluation of tumor extension to the liver (allowing the performance of a EUS-guided FNA for cyto-histological confirmation), peritoneum and/or pleura (with the possibility to perform a EUS-guided FNA of ascites or pleural effusion) (55-61).
CYTO-Histological confirmation of pancreatic tumors
From an oncologist's point of view, it is necessary to obtain a cytological or histological sample in order to confirm the diagnosis of pancreatic adenocarcinoma when the patient requires chemotherapy and/or radiotherapy, or whenever the possibility of neoadjuvant treatment is present (62-64). However, many authors accept other indications to reach a histological confirmation of pancreatic adenocarcinoma in the presence of a pancreatic mass. Among them, the ability to identify lesions other than pancreatic adenocarcinoma, like lymphoma, pancreatic metastasis, autoimmune pancreatitis or an inflammatory mass in chronic pancreatitis, because these lesions require completely different treatments; there is also the possibility of additional information that may assist in preoperative patient and family counseling and therapy selection, as is the case with other tumors(65,66).
In this context, EUS-guided FNA has proven be an essential tool because of its high accuracy and minimum complications (Fig. 3). In the studies published in the literature, the diagnostic accuracy of EUS-guided FNA ranges between 72 and 96% (67-79). Among them, we will focus on the most complete papers. In the study by Harewood et al. (76), prospectively including 185 consecutive patients with the suspicion of pancreatic cancer, all patients underwent a CT scan (61 with CT-guided FNA) and 91 ERPC (41 of them with cytology). In 58 patients with a negative cytology after CT-guided FNA, EUS-guided FNA showed a sensitivity for malignancy of 90%. Similarly, in 36 patients with a negative cytology at ERCP, the diagnostic sensitivity for malignancy with EUS-guided FNA was 94%. Eloubeidi et al. performed a study prospectively including 158 patients with the suspicion of pancreatic cancer. With a median of 3 passes, the diagnostic sensitivity, specificity and overall accuracy of EUS-guided FNA was 84.3, 97, and 84%, respectively (78).

EUS-guided FNA, apart from determining whether a lesion is benign or malignant, also allows a definitive diagnosis to be established. Iglesias-García et al. (80), in a prospective study including 62 consecutive patients with pancreatic solid tumors, were able to diagnose lesions other than pancreatic adenocarcinoma, like lymphoma, oat-cell metastasis from lung cancer, anaplastic carcinoma, and up to 24 inflammatory masses. The overall diagnostic accuracy obtained was 90.2%. However, the most important point in this setting was the differential diagnosis with chronic pancreatitis and autoimmune pancreatitis. In this context, EUS-guided FNA has also shown a high accuracy (81-84). Varadarajulu et al. (82), in a study including 282 patients with pancreatic solid tumors with and without chronic pancreatitis, EUS-guided FNA showed a lower diagnostic sensitivity in the group of patients with chronic pancreatitis (73.9 vs. 91.3%; p = 0.02). There were no differences in terms of specificity (100 vs. 93.8%) and overall accuracy (91.5 vs. 91.4%). In another study published by Ardengh et al. (83), including 69 pancreatic masses in chronic pancreatitis, EUS-guided FNA increased diagnostic sensitivity, specificity and overall accuracy in the differential diagnosis between inflammatory conditions and pancreatic adenocarcinoma (72.7 vs. 63.6%; 100 vs. 75.9%; 95.7 vs. 73.9%; respectively).
However, the best study, in terms of design and final conclusions, is the one published by Eloubeidi et al. (84) - 547 patients who underwent EUS-guided FNA over a 4.5-year period were enrolled. Patients underwent surgical exploration and resection based on their comorbidity status, and on evidence of resectability based on spiral computed tomography (CT) and EUS imaging reviewed in a multidisciplinary approach. The operating characteristics of EUS-guided FNA for solid pancreatic masses were: sensitivity 95% (95% CI: 93.2-95.4), specificity 92% (95% CI: 86.6-95.7), positive predictive value 98% (95% CI: 97-99), negative predictive value 80% (95% CI: 74.9-82.7). The overall accuracy of EUS-guided FNA was 94.1% (95% CI: 92.0-94). Of the 414 true positive patients according to EUS-guided FNA, 138 (33%) were explored; 82% of true positive patients were ultimately found inoperable and received palliative therapy or chemotherapy. They concluded that EUS-guided FNA is a safe and highly accurate method for tissue diagnosis in suspected pancreatic cancer. This approach allows for a preoperative counseling of patients, minimizing surgeon's operative time in cases of unresectable disease, and avoids surgical biopsies in a majority of patients with inoperable disease. However, they recommend a surgical exploration of patients with a clinical scenario suspicious for pancreatic cancer - a mass found on EUS or CT, but inconclusive or negative cytology.
Finally, in the study published by Lambert et al. (85), EUS-guided FNA had important clinical implications for patient management; in fact, it can contraindicate surgical procedures in 41% of patients, avoid the performance of other diagnostic techniques in 57% of cases, and modify the therapeutic attitude in 68% of cases.
But a crucial point of EUS-guided FNA is the low rate of complications associated with the technique. The risk of bacteremia is very low; the risk of acute pancreatitis ranges from 1 to 2%, and the probability of bleeding or peritonitis is rare. The group of cystic lesions is more dangerous, mainly due to the risk of infection; therefore, antibiotics are always recommended following pancreatic cyst aspiration (86). The largest study included 355 patients who underwent EUS-guided FNA for solid pancreatic lesions. Major complications were encountered in 9 patients (2.54%, 95% CI 1.17-4.76). Acute pancreatitis occurred in 3 of 355 (0.85%, 95% CI 0.17-2.45); 2 patients were hospitalized, and 1 patient recovered with outpatient analgesics. Three patients were admitted for severe pain after the procedure; all were treated with analgesics and subsequently discharged with no sequels. Two patients (0.56%, 95% CI 0.07-2.02) developed fever and were admitted for intravenous antibiotics; one patient recovered with intravenous antibiotics and the other required surgical debridement for necrosis. One patient required the use of reversal medication. Overall, 1.97% (95% CI 0.80-4.02) of patients was hospitalized for complications. None of the patients experienced clinically significant hemorrhage, perforation, or death (87). The rate of tumoral seeding with EUS-guided fine-needle aspiration is significantly lower than with percutaneous-guided fine-needle aspiration. In the paper published by Micames et al., in the EUS-guided FNA group only one patient out of 46 developed peritoneal carcinomatosis, compared to 7 out of 43 in the percutaneous-guided FNA group (2.2 vs. 16.3%; p < 0.025). The authors recommended EUS-guided FNA as the method of choice for diagnosis in patients with potentially resectable pancreatic cancer (88).
Conclusions
We can conclude that EUS is superior to other imaging techniques for the detection of pancreatic tumors, mainly in small pancreatic solid lesions. EUS seems to be superior to other imaging procedures for local staging (T), mainly in the evaluation of vascular invasion of the portal vein and splenic vessels. However, EUS seems to be equivalent to the other imaging techniques (mainly CT scan) in the evaluation of nodal staging and overall vascular invasion, and in the assessment of tumor resectability. However, it is important to point out that EUS is clearly operator-dependent, and in very experienced hands its accuracy is very high; new multidetector-row CT equipments have been developed recently, which may probably be similar in terms of accuracy to EUS.
EUS-guided FNA is also becoming essential in the management of pancreatic cancer, mainly related to its high accuracy and low morbidity and mortality. At present, a diagnosis of pancreatic adenocarcinoma must be confirmed when the patient requires chemotherapy and/or radiotherapy, or whenever the possibility of neoadjuvant treatment is present. It is also very important that conditions other than pancreatic adenocarcinoma, which require specific treatment, be identified.
References
1. Jemal A, Murray T, Ward E, Samuels A, Tiwari RC, Ghafoor A, et al. Cancer statistics, 2005. CA Cancer J Clin 2005; 55: 10-30. [ Links ]
2. Williamson RCN. Pancreatic cancer: the greatest oncological challenge. Br Med J 1988; 296: 445-6. [ Links ]
3. Trede M, Schwall G, Saeger HD. Survival after pancreatoduodenectomy: 118 consecutive resections without an operative mortality. Ann Surg 1990; 211: 447-58. [ Links ]
4. Warshaw AL, Gu ZY, Wittenberg J, Walkman AC. Preoperative stanging and assessment of resectability of pancreatic cancer. Arch Surg 1990; 125: 230-3. [ Links ]
5. ASGE Standards of Practice Committee, Gan SI, Rajan E, Adler DG, Baron TH, Anderson MA, et al. Role of EUS. Gastrointest Endosc 2007; 66(3): 425-34. [ Links ]
6. Boujaoude J. Role of endoscopic ultrasound in diagnosis and therapy of pancreatic adenocarcinoma. World J Gastroenterol 2007; 13(27): 3662-6. [ Links ]
7. Yasuda K, Mukai H, Fujimoto S, Nakajima M, Kawai K. The diagnosis of pancreatic cancer by endoscopic ultrasonography. Gastrointest Endosc 1988; 34: 1-8. [ Links ]
8. Rösch T, Lorenz R, Braig C, Feuerbach S, Siewert JR, Schusdziarra V, et al. Endoscopic ultrasound in pancreatic tumor diagnosis. Gastrointest Endosc 1991; 37: 347-52. [ Links ]
9. Rosch T, Braig C, Gain T, Feuerbach S, Siewert JR, Schusdziarra V, et al. Staging of pancreatic and ampullary carcinoma by endoscopic ultrasonography: comparison with conventional sonography, computed tomography, and angiography. Gastroenterology 1992; 102: 188-99. [ Links ]
10. Snady H, Cooperman A, Siegel J. Endocopic ultrasonography compared with computed tomography with ERCP in patients with obstructive jaundice or small peri-pancreatic mass. Gastrointest Endosc 1992: 38: 27-34. [ Links ]
11. Palazzo L, Roseau G, Gayet B, Vilgrain V, Belghiti J, Fékéte F, et al. Endoscopic ultrasonography in the diagnosis and staging of pancreatic adenocarcinoma: results of a prospective study with comparison to ultrasonography and CT scan. Endoscopy 1993; 25: 143-150. [ Links ]
12. Müller MF, Meyenberger C, Bertschinger P, Schaer R, Marincek B. Pancreatic tumors: evaluation with endoscopic US, CT, and MR imaging. Radiology 1994; 190: 745-51. [ Links ]
13. Marty O, Aubertin JM, Bouillot JL, Hernigou A, Bloch F, Petite JP. Prospective comparison of ultrasound endoscopy and computed tomography in the assessment of locoregional invasiveness of malignant ampullary and pancreatic tumors verified surgically. Gastroenterol Clin Biol 1995; 19: 197-203. [ Links ]
14. Melzer E, Avidan B, Hayman Z, Coret A, Bar-Meir S. Preoperative assessment of blood Wessel involvement in patients with pancreatic cancer. Isr J Med Sci 1996; 32: 1086-8. [ Links ]
15. Dufour B, Zins M, Vilgrain V, Levy P, Bernades P, Menu Y. Comparison between spiral X-ray computed tomography and endosonography in the diagnosis and staging of adenocarcinoma of the pancreas. Clinical preliminary study. Gastroenterol Clin Biol 1997; 21: 124-30. [ Links ]
16. Howard TJ, Chin AC, Streib EW, Kopecky KK, Wiebke EA. Value of helical computed tomography, angiography and endoscopic ultrasound in determining resectability of periampullary carcinoma. Am J Surg 1997; 174: 237-41. [ Links ]
17. Sugiyama M, Hagi H, Atomi Y, Saito M. Diagnosis of portal venous invasion by pancreatobiliary carcinoma: value of endoscopic ultrasonography. Abdom Imaging 1997; 22: 434-8. [ Links ]
18. Legmann P, Vignaux O, Dousset B, Baraza AJ, Palazzo L, Dumontier I, et al. Pancreatic tumors: comparison of dual phase helical CT and endoscopic sonography. AJR Am J Roentgenol 1998; 170: 1315-22. [ Links ]
19. Akahoshi K, Chijiiwa Y, Nakano I, Nawata H, Ogawa Y, Tanaka M, et al. Diagnosis and staging of pancreatic cancer by endoscopic ultrasound. Br J Radiol 1998; 71: 492-6. [ Links ]
20. Harrison JL, Millikan KW, Prinz RA, Zaidi S. Endoscopic ultrasound for diagnosis and staging of pancreatic tumors. Am Surg 1999; 65: 659-65. [ Links ]
21. Gress FG, Hawes RH, Savides TJ, Ikenberry SO, Cummings O, Kopecky K, et al. Role of EUS in the preoperative staging of pancreatic cancer: a large single-center experience. Gastrointest Endosc 1999; 50: 786-91. [ Links ]
22. Midwinter MJ, Beveridge CJ, Wilsdon JB, Bennett MK, Baudouin CJ, Charnley RM, et al. Correlation between spiral computed tomography, endoscopic ultrasonography and findings at operation in pancreatic and ampullary tumours. Br J Surg 1999; 86: 189-93. [ Links ]
23. Mertz HR, Sechopoulos P, Delbeke D, Leach SD. EUS, PET and CT scanning for evaluation of pancreatic adenocarcinoma. Gastrointest Endosc 2000; 52: 367-71. [ Links ]
24. Rivadeneira DE, Pochapin M, Grobmyer SR, Lieberman MD, Christos PJ, Jacobson I, et al. Comparison of linear array endoscopic ultrasound and helical computed tomography for the staging of periampullary malignancies. Ann Surg Oncol 2003; 10: 890-7. [ Links ]
25. Ainsworth AP, Rafaelsen SR, Wamberg PA, Durup J, Pless TK, Mortensen MB. Is there a difference in diagnostic accuracy and clinical impact between endoscopic ultrasonography and magnetic resonante cholangiopancreatopgraphy? Endoscopy 2003; 35: 1029-32. [ Links ]
26. Agarwal B, Abu-Hamda E, Molke KL, Correa AM, Ho L. Endoscopic ultrasound guided fine needle aspiration and multidetector spiral CT in the diagnosis of pancreatic cancer. Am J Gastroenterol 2004; 99: 844-850. [ Links ]
27. DeWitt J, Devereaux B, Chriswell M, McGreevy K, Howard T, Imperiale TF, et al. Comparison of endoscopic ultrasound and multidetector computed tomography for the detection and staging of pancreatic cancer. Ann Intern Med 2004; 141: 753-63. [ Links ]
28. Ardengh JC, de Paulo GA, Ferrari AP. Pancreatic carcinomas smaller than 3.0 cm: endosonography (EUS) in diagnosis, staging and prediction of resectability. HPB (Oxford) 2003; 5(4): 226-230. [ Links ]
29. Bronstein YL, Loyer EM, Kaur H, Choi H, David C, DuBrow RA, et al. Detection of small pancreatic tumors with multiphasic helical CT. AJR Am J Roentgenol 2004; 182: 619-23. [ Links ]
30. Agarwal B, Krishna NB, Labundy JL, Safdar R, Akduman EI. EUS and/or EUS-guided FNA in patients with CT and/or magnetic resonance Imaging findings of enlarged pancreatic head or dilated pancreatic duct with or without a dilated common bile duct. Gastrointest Endosc 2008; 68: 237-42. [ Links ]
31. Sing S, Reddymassu S, Waheed S, Vail M, He J, Talapaneni J, et al. Endoscopic ultrasonography findings in patients with non-specific changes of the pancreas on computed tomography: a single center experience. Dig Dis Sci 2008; 53: 2799-804. [ Links ]
32. Catanzaro A, Richarson S, Veloso H, Isenberg GA, Wong RC, Sivak MV Jr., et al. Long-term follow-up of patients with clinical indetermine suspicion of pancretic cancer and normal EUS. Gastrointest Endosc 2003; 58: 836-40. [ Links ]
33. DeWitt J, DeverauxBM, Lehman GA, Sherman S, Imperiale TF. Comparison of Endoscopic Ultrasound and Computed Tomography for the Preoperative Evaluation of pancretic cancer: A systematic review. Clin Gastroenterol Hepatol 2006; 4: 717-25. [ Links ]
34. Tio TL, Tytgat GN, Cikot RJ, Houthoff HJ, Sars PR. Ampullopancreatic carcinoma: preoperative TNM classification with endosonography. Radiology 1990; 175: 455-61. [ Links ]
35. Yasuda K, Mukai H, Nakajima M, Kawai K. Staging of pancreatic carcinoma by endoscopic ultrasonography. Endoscopy 1993; 25: 151-5. [ Links ]
36. Giovannini M, Seitz JF. Endoscopic ultrasonography with linear-type echoendoscope in the evaluation of 94 patients wit pancreaticobiliay disease. Endoscopy 1994; 26: 579-85. [ Links ]
37. Tio TL, Sie LH, Kallimanis G, Luiken GJ, Kimmings AN, Huibregtse K, et al. Staging of ampullary and pancreatic adenocarcinoma: comparison between endosonography and surgery. Gastrointest Endosc 1996; 44: 706-13. [ Links ]
38. Buscail L, Pages P, Berthelemy P, Fourtanier G, Frexinos J, Escourrou J. Role of EUS in the management of pancreatic and ampullary carcinoma: a prospective study assessing resectability and prognosis. Gastrointest Endosc 1999; 50: 34-40. [ Links ]
39. Ahmad NA, Lewis JD, Ginsberg GG, Rosato EF, Morris JB, Kochman ML. EUS in preoperative staging of pancreatic cancer. Gastrointest Endosc 2000; 52: 463-8. [ Links ]
40. Seicean A, Badea R, Mocan T, Iancu C, Pop T, Seicean R, Mo Scedil Teanu O, et al. Radial endoscopic ultrasonography in the preoperative staging of pancreatic cancer. J Gastrointest Liver Dis 2008; 17: 273-8. [ Links ]
41. Soriano A, Castells A, Ayuso C, Ayuso JR, de Caralt MT, Ginès MA, et al. Preoperative staging and tumor resectability assessment of pancreatic cancer: prospective study comparing endoscopic ultrasonography, helical computed tomography, magnetic resonance imaging, and angiography. Am J Gastroenterol 2004; 99: 492-501. [ Links ]
42. Ramsay D, Marshall M, Song S, Zimmerman M, Edmunds S, Yusoff I, et al. Identification and staging of pancreatic tumours using computed tomography, endoscopic ultrasound and mangafodipir trisodium-enhanced magnetic resonante imaging. Australas Radiol 2004; 48: 154-61. [ Links ]
43. Tamm EP, Silverman PM, Charnsangavej C, Evans DB. Diagnosis, staging, and surveillance of pancreatic cancer. AJR AM J Roentgenol 2003; 180: 1311-23. [ Links ]
44. Vargas R, Nino-Murica M, Trueblood W, Jeffrey RB Jr. MDCT in pancreatic adenocarcinoma: prediction of vascular invasion and resectability using a multiphasic technique with curved planar reformations. AJR Am J Roentgenol 2004; 182: 419-25. [ Links ]
45. Schick V, Franzius C, Beyna T, Oei ML, Schnekenburger J, Weckesser M, Domschke W, et al. Diagnostic impacto f (18)F-FDG PET-T evaluating solid pancreatic lesions versus endosonography, endoscopic retrograde cholangio-pancreatography with intraductal ultrasonography and abdominal ultrasound. Eur J Nucl Mol Imaging 2008; 35: 1775-85. [ Links ]
46. Lariño-Noia J, Iglesias-García J, Villanueva-Rodríguez A, Iglesias-Canle J, Domínguez-Muñoz JE. Endoscopic ultrasonography vs helical CT for locoregional staging of pancreatic cancer: a prospective comparative trial using histology as gold standard. Pancreatology 2004; 4: 146. [ Links ]
47. Tierney WM, Francis IR, Eckhauser F, Elta G, Nostrant TT, Scheiman JM. The accuracy of EUS and helical CT in the assessment of vascular invasion by peripapillary malignancy. Gastrointest Endosc 2001; 53: 182-8. [ Links ]
48. Brugge WR, Lee MJ, Kelsey PB, Schapiro RH, Warshaw AL. The use of EUS to diagnose malignant portal venous system invasión by pancreatic cancer. Gastrointest Endosc 1996; 43: 561-7. [ Links ]
49. Rosch T, Dittler H-J, Strobel K, Meining A, Schusdziarra V, Lorenz R, et al. Endoscopic ultrasound criteria for vascular invasion in the staging of cancer of the head of the pancreas: a blind reevaluation of videotapes. Gastrointest Endosc 2000; 52: 469-77. [ Links ]
50. Puli SR, Singh S, Hagedorn CH, Reddy J, Olyaee M. Diagnostic accuracy of EUS for vascular invasion in pancreatic and periampullary cancers: A meta-analysis and systematic review. Gastrointest Endosc 2007; 65(6): 788-97. [ Links ]
51. Nakaizumi A, Uehara H, Iishi H, Tatsuta M, Kitamura T, Kuroda C, et al. Endoscopic ultrasonography in the diagnosis and staging of pancreatic cancer. Dig Dis Sci 1995; 40: 696-700. [ Links ]
52. Cahn M, Chang K, Nguyen P, Butler J. Impact of endoscopic ultrasound with fine needle aspiration on the surgical Management of pancreatic cancer. Am J Surg 1996; 172: 470-2. [ Links ]
53. Hahn M, Faigel DO. Frecuency of mediastinal lymph node metastases in patients undergoing EUS evaluation of pancreaticobiliary masses. Gastrointest Endosc 2001; 54: 331-5. [ Links ]
54. Ahmad NA, Lewis JD, Siegelman ES, Rosato EF, Ginsberg GG, Kochman ML. Role of endoscopic ultrasound and magnetic resonance Imaging in the preoperative staging of pancreatic adenocarcinoma. Am J Gastroenterol 2000; 95: 1926-31. [ Links ]
55. Nguyen P, Feng JC, Chang KJ. Endoscopic ultrasound (EUS) and EUS-guided fine needle aspiration of liver lesions. Gastrointest Endosc 1999; 50: 357-61. [ Links ]
56. DeWitt J, Leblanc J, McHenry L, Ciaccia D, Imperiale T, Chappo J, et al. Endoscopic ultrasound-guided fine needle aspiration cytology of solid liver lesions: a large single-center experience. Am J Gastroenterol 2003; 98: 1976-81. [ Links ]
57. Prasad P, Schulewitz N, Patel A, Varadarajulu S, Wildi SM, Roberts S, et al. Detection of occult liver metastases during EUS for staging of malignancies. Gastrointest Endosc 2004; 59: 49-53. [ Links ]
58. Tenberge J, Hoffman BJ, Hawes RH, Van Enckebort C, Giovannini M, et al. EUS-guided fine needle aspiration of the liver: indications, yield, and safety base don an International Surrey of 167 cases. Gastrointest Endosc 2002; 55: 859-62. [ Links ]
59. Hollerbach S, Willert J, Topalidis T, Reiser M, Schmiegel W. Endoscopic ultrasound-guided fine needle aspiration biopsy of liver lesions: histologicall and cytological assessment. Endoscopy 2003; 35: 743-9. [ Links ]
60. Chang KJ, Albers CG, Nguyen P. Endoscopic ultrasound guided fine needle aspiration of pleural and ascitis fluid. Am J Gastroenterol 1995; 90: 148-50. [ Links ]
61. Nguyen PT, Chang KJ. EUS in the detection of ascites and EUS-guided paracentesis. Gastrointest Endosc 2001; 54: 336-9. [ Links ]
62. American Gastroenterological Association medical position statement: epidemiology, diagnosis, and treatment of pancreatic ductal adenocarcinoma. Gastroenterology 1999; 117(6): 1463-84. [ Links ]
63. Lockhart AC, Rothenberg ML, Berlin JD. Treatment for pancreatic cancer: Current therapy and continued progress. Gastroenterology 2005; 128(6): 1642-54. [ Links ]
64. Wray CJ, Ahmad SA, Matthews JB, Lowy AM. Surgery for pancreatic cancer: Recent controversies and current practice. Gastroenterology 2005; 128(6): 1626-41. [ Links ]
65. Iglesias García J, Domínguez-Muñoz JE. Endoscopic ultrasound-guided biopsy for the evaluation of pancreatic tumors. Gastroenterol Hepatol 2007; 30(10): 597-601. [ Links ]
66. Chang KJ. State of the art lecture: endoscopic ultrasound (EUS) and FNA in pancreatico-biliary tumors. Endoscopy 2006; 38(Supl. 1): S56-60. [ Links ]
67. Giovannini M, Seitz JF, Monges F, Perrier H, Rabbia I. Fine-needle aspiration cytology guided by endoscopic ultrasonography: results in 141 patients. Endoscopy 1995; 27: 171-7. [ Links ]
68. Bhutani MS, Hawes RH, Baron PL, Sanders-Cliette A, van Velse A, Osborne JF, et al. Endoscopic ultrasound guided fine needle aspiration of malignant pancreatic lesions. Endoscopy 1997; 29: 854-8. [ Links ]
69. Gress FG, Hawes RH, Savides TJ, Ikenberry SO, Lehman GA. Endoscopic ultrasound-guided fine-needle aspiration biopsy using linear array and radial scanning endosonography. Gastrointest Endosc 1997; 45: 243-50. [ Links ]
70. Chang KJ, Nguyen P, Erickson RA, Durbin TE, Katz KD. The clinical utility of endoscopic ultrasound-guided fine-needle aspiration in the diagnosis and staging of pancreatic carcinoma. Gastrointest Endosc 1997; 45: 387-93. [ Links ]
71. Faigel DO, Ginsberg GG, Bentz JS, Gupta PK, Smith DB, Kochman ML. Endoscopic ultraosound-guided real-time fine-needle aspiration biopsy of the pancreas in cancer patients with pancreatic lesions. J Clin Oncol 1997; 15: 1439-43. [ Links ]
72. Wiersema MJ, Vilmann P, Giovannini M, Chang KJ, Wiersema LM. Endosonography-guided fine-needle aspiration biopsy: diagnostic accuracy and complication assessment. Gastroenterology 1997; 112: 1087-95. [ Links ]
73. Williams DB, Sahai AV, Aabakken L, Penman ID, van Velse A, Web J. Endoscopic ultrasound guided fine needle aspiration biopsy: a large single center experience. Gut 1999; 44: 720-6. [ Links ]
74. Voss M, Hammel P, Molas G, Palazzo L, Dancour A, O'Toole D. Value of endoscopic ultrasound guided fine needle aspiration biopsy in the diagnosis of solid pancreatic masses. Gut 2000; 46: 244-9. [ Links ]
75. Gress F, Gottlieb K, Sherman S, Lehman G. Endoscopic ultrasonography-guided fine needle aspiration biopsy of suspected pancreatic cancer. Ann Inter Med 2001; 134: 459-64. [ Links ]
76. Harewood GC, Wiersema MJ. Endosonography-guided fine needle aspiration biopsy in the evaluation of pancreatic masses. Am J Gastroenterol 2002; 97: 1386-91. [ Links ]
77. Raut CP, Grau AM, Staerkel GA, Kaw M, Tamm EP, Wolff RA. Diagnostic accuracy of endoscopic ultrasound-guided fine-needle aspiration in patients with presumed pancreatic cancer. J Gastrointest Surg 2003; 7: 118-26. [ Links ]
78. Eloubeidi MA, Chen VK, Eltoum IA, Jhala D, Chhieng DC, Jhala N, et al. Endoscopic ultrasound-guided fine needle aspiration biopsy of patients with suspected pancreatic cancer: diagnostic accuracy and acute and 30-days complications. Am J Gastroenterol 2003; 98(12): 2663-8. [ Links ]
79. Ardengh JC, Lopes CV, Pereira de Lima LP, Rodrigues de Oliveira J, Venco F, Santo GC, et al. Diagnosis of pancreatic tumors by endoscopic ultrasound-guided fine-needle aspiration. World J Gastroenterol 2007; 13 (22): 3112-6. [ Links ]
80. Iglesias-García J, Domínguez-Muñoz JE, Lozano-León A, Abdulkader I, Lariño-Noia J, Antúnez J, et al. Impact of endoscopic-ultrasound fine needle biopsy for diagnosis of pancreatic masses. World J Gastroenterol 2007; 13(2): 289-93. [ Links ]
81. Takahashi K, Yamao K, Okubo K, Sawaki A, Mizuno N, Ashida R, et al. Differential diagnosis of pancreatic cancer and focal pancreatitis by using EUS-guided FNA. Gastrointest Endosc 2005; 61: 76-9. [ Links ]
82. Varadarajulu S, Tambane A, Eloubeidi MA. Yield of EUS-guided FNA of pancreatic masses in the presence or the absence of chronic pancreatitis. Gastrointest Endosc 2005; 62: 728-36. [ Links ]
83. Ardengh JC, Lopes CV, Campos AD, Pereira de Lima LF, Venco F, Módena JL. Endoscopic ultrasound and fine needle aspiration in chronic pancreatitis. Differential Diagnosis between pseudotumoral masses and pancreatic cancer. J Pancreas 2007; 8: 413-21. [ Links ]
84. Eloubeidi MA, Varadarajulu S, Desai S, Shirley R, Heslin MJ, Mehra M, et al. A prospective evaluation of an algorithm incorporating routine preoperative endoscopic ultrasound-guided fine needle aspiration in suspected pancreatic cancer. J Gastrointest Surg 2007; 11(7): 813-9. [ Links ]
85. Lambert R, Caletti G, Cho E, Chang KJ, Fusaroli P, Feussner H, et al. International Workshop on the clinical impact of endoscopic ultrasound in gastroenterology. Endoscopy 2000; 32: 549-84. [ Links ]
86. Adler DG, Jacobson BC, Davila RE, Hirota WK, Leighton JA, Qureshi WA, Rajan E, ASGE. ASGE guidelines: complications of EUS. Gastrointest Endosc 2005; 61: 8-12. [ Links ]
87. Eloubeidi MA, Tamhane A, Varadajulu S. Frequency of major complications after EUS-guided FNA of solid pancreatic masses: a prospective evaluation. Gastrointest Endosc 2006; 63: 622-9. [ Links ]
88. Micames C, Jowell PS, White R, Paulson E, Nelson R, Morse M, et al. Lower frequency of peritoneal carcinomatosis in patients with pancreatic cancer diagnosed by EUS-guided FNA vs percuteneous FNA. Gastrointest Endosc 2003; 58: 690-5. [ Links ]
![]() Correspondence:
Correspondence:
Julio Iglesias García.
Gastroenterology Department.
Foundation for Research in Digestive Diseases.
University Hospital of Santiago de Compostela.
C/ Choupana, s/n. 15706 Santiago de Compostela, Spain.
e-mail: julioiglesiasgarcia@hotmail.es
Received: 17-03-09.
Accepted: 18-03-09.

