










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.101 n.9 Madrid Sep. 2009
PICTURES IN DIGESTIVE PATHOLOGY
Small bowel perforation by an unusual foreign body
Perforación de intestino delgado por un inusual cuerpo extraño
J. I. Rodríguez-Hermosa, N. Cañete1, E. Artigau, J. Gironès, P. Planellas and A. Codina-Cazador
Departments of General and Digestive Surgery, and 1Radiology. University Hospital Dr. Josep Trueta. Girona, Spain
Introduction
Although accidental ingestion of foreign bodies is a common problem in the general population, most objects pass through the entire digestive tract without incidents (1). However, in 1% of cases, it causes complications such as acute abdomen due to intestinal perforation (2). In some cases, it can cause severe complications and even death; in the USA, 1,500 people die annually from foreign body ingestion (3).
Case report
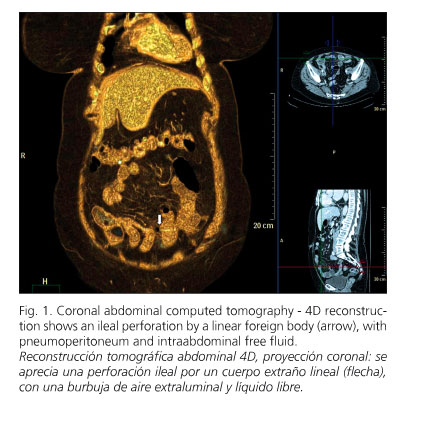
A 73-year-old woman with comorbid conditions, including arterial hypertension, hiatal hernia, colonic diverticulosis, urinary infection, and previous abdominal surgery (hysterectomy) presented at the emergency department with diffuse abdominal pain with peritoneal irritation and vomiting of 24 hours' duration. Laboratory tests showed slight leukocytosis (11,600/mm3) and increased C-reactive protein (19 mg/dl). Abdominal CT showed a foreign body in the small bowel, with pneumoperitoneum and fluid within the abdominal cavity (Fig. 1). After median laparotomy, a 2-mm ileal perforation by a foreign body and diffuse purulent peritonitis were evident in an area with adhesions (Fig. 2). Lysis of the adhesions, removal of the foreign body - a sprig of thyme (Fig. 3) -, primary suture of the intestinal perforation, and abdominal cavity lavage were performed. Intravenous ertapenem (1 g/24 h) was administered. The patient, who wore dentures, referred the ingestion of roast chicken 3 weeks before. She was discharged on the sixth day after admission without complications.


Discussion
Generally, the ingestion of foreign bodies occurs involuntarily while eating; meat boluses are the most common foreign bodies ingested in western countries, and fish bones in oriental countries (2-4).
One predisposing risk factor for foreign body ingestion is the use of dentures, because they reduce the sensitivity of the palate (2-4).
Areas where perforations by foreign bodies are most frequent include the ileocecal and rectosigmoid regions, because the intestinal lumen narrows and the digestive tract is angulated in these sites. Sites where impaction is most likely include zones with adhesions, areas containing a diverticular process, or surgical anastomoses (2-4).
Treatment consists of surgery (from primary suture to rectosigmoid resection with colostomy, removal of the foreign body, and abdominal cavity lavage), and antibiotics (2-4).
References
1. Ramos R, Duarte P, Vicente C, Casteleiro C. Upper gastrointestinal bleeding triggered by foreign body ingestion. Rev Esp Enferm Dig 2008; 100: 238-9. [ Links ]
2. Rodríguez-Hermosa JI, Codina-Cazador A, Sirvent JM, Martín A, Gironès J, Garsot E. Surgically treated perforations of the gastrointestinal tract caused by ingested foreign bodies. Colorectal Dis 2008; 10: 701-7. [ Links ]
3. Rodríguez-Hermosa JI, Ruiz-Feliú B, Roig-García J, Albiol-Quer M, Planellas-Giné P, Codina-Cazador A. Lethal intestinal perforation after foreign body ingestion in a superobese patient. Obes Surg 2009; 19: 1183-5. [ Links ]
4. Goh BK, Chow PK, Quah HM, Ong HS, Eu KW, Ooi LL, et al. Perforation of the gastrointestinal tract secondary to ingestion of foreign bodies. World J Surg 2006; 30: 372-7. [ Links ]

