










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.101 n.10 Madrid Oct. 2009
LETTERS TO THE EDITOR
Intermittent small bowel obstruction secondary to enterolithiasis in Crohn's disease
Obstrucción intestinal intermitente secundaria a enterolitiasis en enfermedad de Crohn
Key words: Crohn's disease. Intestinal obstruction. Stenosis.
Palabras clave: Enfermedad de Crohn. Obstrucción intestinal. Estenosis.
Dear Editor,
Intestinal obstruction is a common complication of inflammatory bowel disease (IBD), not when their cause is the formation of enteroliths. Enteroliths associated with Crohn's disease is an unusual disease, there are reported in the literature less than 25 cases, we have found just one in Spanish.
We report a case of intestinal obstruction in Crohn's disease secondary to enterolithiasis.
Case report
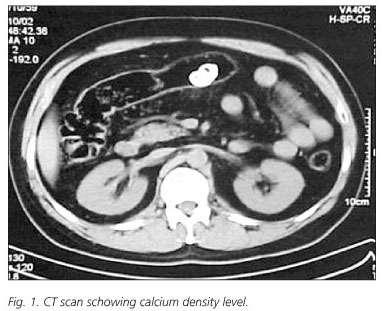
Man of 43 years-old, with no toxic habits, cardiovascular risk factors or previous surgery. He was diagnosed of Crohn's disease 11 years ago localized in ileum and colon, in treatment with mesalazine. Among the tests that were performed along the course of his disease there were two intestinal transits with barium and two colonoscopies. He came to the Emergency Unit for epigastric pain of one month of evolution, becoming continuous and more intense in the last 48 hours, accompanied of abdominal distension, nausea, vomits and constipation. To the physical examination he showed a good general condition, no fever and hemodinamic stability, with a distended abdomen, tympanic, painful to the diffuse palpation and decrease in intestinal persistalsis. Among the complementaries studies there were a hemogram and a general analysis with acute phase reactants that were within normal. In abdominal Rx we saw two rounds images with calcium density level L2-L3 on both sides of the median line. The diagnosis was completed with abdominal CT scan that reported foreign bodies in the transverse colon (Fig. 1). A colonoscopy was performed, that it could not move beyond 100 cm by insuperable stenosis at this level despite we tried dilation. The resolution of the case was not possible by endoscopy. We decided surgery by laparotomy with resection of the stenosis and removal of the stones. The histological examination reported of limestone formations, the first of 17-mm diameter and 15 mm the second (Fig. 2).

Discussion
We know as enterolithes the calculations made by the deposition of mineral salts in concentric layers around a core, usually constituted by non-digestible organic matter. It is a common disease in some animals such as horses, but not in humans. Among the factors involved for their formation is the existence of diverticula, adhesions, narrow segments along the digestive tract, previous examinations with barium and slowed intestinal transit (1-6). The latter is postulated as the main factor in its formation, and in most cases before enterolithiasis there is a long history of IBD. (1.2). These cases, according to some authors should consider us the possibility of an underlying adenocarcinoma (1). They are usually asymptomatic and they are found as an accidental discovery in a test image. Finding suggestive images lithiasis outside their areas, such as kidney or gallbladder, should make us suspect that we are facing an enterolithiasis (2). When the disease is symptomatic it can present as a chronic anemia by digestive bleeding, obstruction, pseudobstruction, intestinal perforation among others (3).
Most enterolithes are radiopaque, easily visible with a simple test of radiology. But we can not discard them with a normal X-ray because some of them are radiolucent (made of magnesium salts). In these cases the study should be completed with CT scan (4,5).
In our patient we find some of those factors reflected in the literature as predisposing to the formation of enterolithes such as long evolution of Crohn's disease, radiological studies with barium and stenosis along the intestinal tract.
Sometimes it is possible the resolution of the case by endoscopic balloon dilation, allowing the stone extraction by endoscopy. This technique is described like a choice in most cases because good results and low complication rate (< 5%). In those cases in which it is not possible, we can conduct the resection of the bowel affected by laparotomy or laparoscopy (6), as in our case.
A. Bejarano García, H. Pallarés Manrique, C. Nuñez Sousa, M. Gata Cuadrado,
M. C. García Esteban, M. Rojas Feria, M. Ramos Lora and A. Domínguez Macías
Unit of Digestive-Surgery Clinical Management. Section of Digestive Diseases. Hospital Juan Ramón Jiménez. Huelva, Spain
References
1. Orts JA, Morell L, Camps J. Traba ML, Belenguer A, Guerrero A. Enterolitiasis múltiple, coexistiendo con litiasis biliar y vesical, asociada a adenocarcinoma de colon. An Med Interna 2005; 22(5): 227-30. [ Links ]
2. Bruni R, Chirco L, Lemeni AR, Petrocca S. Intermittent small bowel obstruction by jejunal enteroliths in a patient with a Crohn's disease stricture. Chir Ital 2002; 54(6): 903-5. [ Links ]
3. Yuan JG, Sachar DB, Koganei K, Greenstein AJ. Enterolithiasis, refractory anemia, and strictures of Crohn's disease. J Clin Gastroenterol 1994; 18(2): 105-8. [ Links ]
4. Mendes Ribeiro HK, Nolan DJ. Enterolithiasis in Crohn's disease. Abdom Imagin 2000; 25(5): 526-9. [ Links ]
5. Geoghegan T, Stunel H, Ridgeway P, Birido N, Geraghty J, Torreggiani WC. Small bowel obstruction secondary to a giant enterolith complicating Crohn's disease. Ir J Med Sci 2005; 174(2): 58-9. [ Links ]
6. Jones MW, Koper B, Weatherhead WF. Crohn's disease with enterolith treated laparoscopically. JSLS 2005; 9(3): 339-41. [ Links ]

