










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.102 n.6 Madrid Jun. 2010
CARTAS AL DIRECTOR
Sengstaken-Blakemore tube related esophageal rupture
Ruptura esofágica asociada a tubo de Sengstaken-Blakemore
Key words: Esophageal rupture. Sengstaken-Blakemore tube.
Dear Editor,
The Sengstaken-Blakemore (SB) tube, which was first described in 1950s (1), is a multiluminal plastic tube with two inflatable balloons. The proximal balloon is used to arrest bleeding by directly compressing the esophageal varices. The effectiveness of balloon tamponade with the SB tube is quoted as 90% (1). Esophageal rupture is a rarely reported fatal complication following treatment of bleeding esophageal varices with the SB tube (2,3). We presented a case of SB tube related esophageal rupture, which was confirmed by CT scan.
Case report
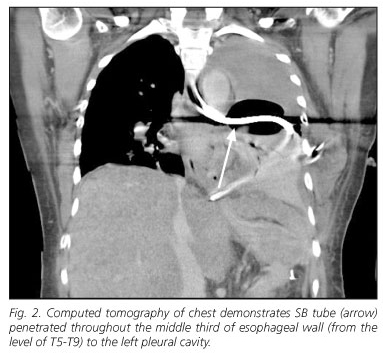
A 51 year old female has alcoholic cirrhosis of liver with esophageal varices for 5 years. She was admitted because of uncontrolled esophageal variceal (EV) bleeding. The patient underwent exp. lap with ligation of esophageal varices, devascularization and splenectomy 3 years ago. The patient presented to the emergency department with a new episode of massive hematemesis with shock, and then admitted to intensive care unit (ICU). An emergent upper gastro-intestinal (GI) endoscopy was performed, which revealed active bleeding from ruptured esophageal varices. She had required placement of a Sengstaken-Blakemore tube for massive EV bleeding with unstable hemodynamic status. A chest radiograph taken soon after insertion of SB tube and showed a malpositioned gastric balloon (Fig. 1). Computed tomography of the chest showed SB tube penetrated throughout the middle third of esophageal wall to the left pleural cavity (Fig. 2). The patient underwent emergent surgical intervention of thoracotomy with repair of ruptured esophagus and cervical esophagostomy. Postoperative course was uneventful, and the patient was well. The patient died of sepsis 6 months later.

Discussion
Esophageal rupture as a complication of management of esophageal varices secondary to portal hypertension was a particularly lethal injury. While balloon tamponade with SB tube is life saving and effective in 60-90% of bleeding esophageal varices (4), it is slowly becoming the least preferred method due to the high incidence of complications. The most common complications include aspiration pneumonia, esophageal or gastric injuries, airway obstruction, tracheal injury and pressure necrosis of the mucosa (4,5).
We report this case and show the importance of proper tube position be confirmed by CT of chest. Although ultrasound confirmed placement of SB tube was raised recently, failure in identifying the gastroesophageal junction sometimes occurs (6). As in our patient, CT scan with sagital and coronal reformations is the more efficient diagnostic modality for confirming the diagnosis of a ruptured esophagus as well as further surgical plans.
It is important to consider the possibility in any patient presenting with atypical chest or abdominal pain after induction of SB tube. Esophageal rupture remains an important thoracic emergency, and accompanied complications include pneumonia, mediastinitis, sepsis, empyema, and respiratory distress syndrome. Aggressive operative therapy remains the mainstay for treatment. The use of CT scan might be more helpful in early detection of esophageal rupture when a chest radiograph is equivocal.
In conclusion, rupture of the esophagus is a critical injury with a high mortality rate. Following insertion of the SB tube, routine chest radiographs should be taken before and after full inflation of the gastric balloon to ascertain correct tube position. In addition, image studies of CT should be obtained immediately to make an accurate diagnosis of a suspected esophageal rupture to prevent further complications and prolonged hospitalization. The prognosis can be poor, especially if diagnosis is delayed. We suggest the early CT scan intervention is more helpful and necessary if SB tube related esophageal rupture is suspected.
C. T. Lin, T. W. Huang, S. C. Lee, S. M. Kuo, K. F. Hsu, P. S. Hsu, H. K. Huang and H. Chang
Division of Thoracic Surgery. Department of Surgery. Tri-Service General Hospital. National Defense Medical Center. Taipei, Taiwan
References
1. Sengstaken RW, Blakemore AH. Balloon tamponage for the control of hemorrhage from esophageal varices. Ann Surg 1950; 131: 781-9. [ Links ]
2. Hamm DD, Papp JP. Rupture of esophagus during use of Sengstaken-Blakemore tube. Postgrad Med 1974; 56: 199-200. [ Links ]
3. Zeid SS, Young PC, Reeves JT. Rupture of the esophagus after introduction of the Sengstaken-Blakemore tube. Gastroenterology 1959; 36: 128-31. [ Links ]
4. Gossat D, Bolin TD. An unusual complication of balloon tamponade in the treatment of esophageal varices: a case report and brief review of the literature. Am J Gastroenterol 1985; 80: 600-1. [ Links ]
5. Vlavianos P, Gimson AE, Westaby D, Williams R. Balloon tamponade in variceal bleeding: use and misuse. BMJ 1989; 298: 1158. [ Links ]
6. Lin AC, Hsu YH, Wang TL, Chong CF. Placement confirmation of Sengstaken-Blakemore tube by ultrasound. Emerg Med J 2006; 23(6): 487. [ Links ]

