










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.102 no.11 Madrid nov. 2010
PICTURES IN DIGESTIVE PATHOLOGY
Endoscopic retrieval of a surgical gauze from the right colon
Extracción endoscópica de gasa quirúrgica en colon derecho
J. B. Gornals-Soler, T. Lobatón-Ortega, F. Rodríguez-Moranta and J. Miquel-Collell
Unidad de Endoscopia. Servicio Aparato Digestivo. Hospital Universitari de Bellvitge. Barcelona, Spain
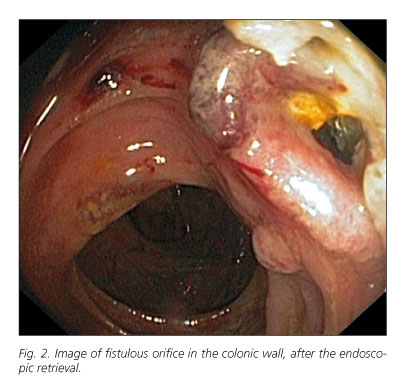
A 33-year-old man, who had been operated on a congenital bridle 14 years ago, was admitted to our hospital for evaluation of a 3 month recurrent abdominal pain. CT scan and colonoscopy were performed in another medical centre, in which a chronic inflammatory process surrounding a foreign body was described in the right colon. He was referred to our endoscopy unit, as a tertiary reference hospital, in order to evaluate its extraction. During the endoscopic procedure was visualized a surgical gauze wrapped to an inflammatory intestinal mucosa (with edema and friability) and externalized to the colon lumen (Fig. 1). Using an endoscopic grasping forceps it was slowly removed until its complete extraction, with a 60 cm total length (Fig. 2). It revealed a fistulous orifice (Fig. 3) which was communicated with a cavity, without any evidence of active haemorrhage. He had a good clinical evolution and outcome; no more episodes of abdominal pain were referred. A control CT scan was performed 3 months later, which showed slight residual inflammatory changes. It is not unusual to find surgical foreign bodies after a surgical intervention (1,2). They are usually symptomatic; presenting as abscesses, acute or chronic abdominal pain or haemorrhage, due to blood vessels or intestinal wall's erosion. Normally, the therapeutic approach consists in another surgical intervention in order to remove the foreign body (3). In our particular case, symptoms revealed 14 years after the surgical intervention. In our opinion, it is striking the natural evolution of the foreign body to show its way out to the intestinal lumen. In this case, the endoscopic procedure avoided surgery by helping the gauze's extraction.


References
1. Cipolletta L, Bianco MA, Rotondano G, Prisco A, Catalano M, Gatto A, Carlomagno P. Endoscopic retrieval of a surgical gauze from the common bile duct. Ital J Gastroenterol Hepatol 1997; 29(1): 58-61. [ Links ]
2. Ibrahim IM. Retained surgical sponge. Surg Endosc 1995; 9(6): 709-10. [ Links ]
3. Childers JM, Caplinger P. Laparoscopic retrieval of a retained surgical sponge: a case report. Surg Laparosc Endosc 1993; 3(2): 135-8. [ Links ]

