










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.103 no.5 Madrid may. 2011
https://dx.doi.org/10.4321/S1130-01082011000500008
PICTURES IN DIGESTIVE PATHOLOGY
Large asymptomatic type III paraesophageal hernia
Gran hernia hiatal paraesofágica tipo III asintomática
Carlos Castaño-Milla, Enrique de la Fuente-Fernández and Luisa García-Buey
Departments of Gastroenterology and Hepatology. Hospital Universitario de La Princesa. Madrid, Spain
Introduction
Hiatal hernias involve the herniation of part of abdominal contents through the esophageal hiatus of the diaphragm. There are four types: type I or sliding hiatal hernia, type II or paraesophageal hiatal hernia, or mixed type III and type IV, in which ascend to the chest organs like the colon and spleen (1).


Clinical observation
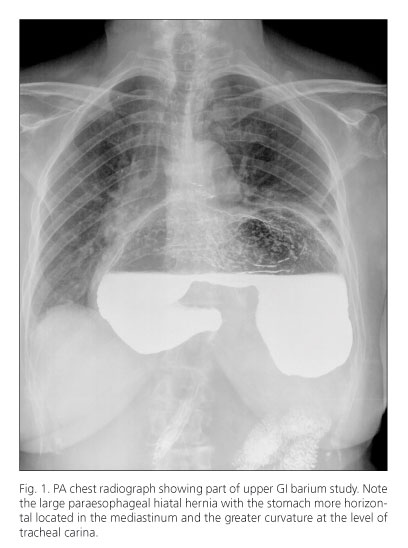
A 67 year-old-woman was admitted to the Gastroenterology Department to study microcytic anemia, and heartburn. She had a hemoglobin of 6.4 g/dL, MCV 61 m3 and profile of iron deficiency. We performed a gastroscopy, which revealed a large hiatal hernia with a mixed component and a tarnished mucosa in the fundus, antrum and body. The barium radiological study demonstrated a horizontalization of the stomach in the mediastinum, with the gastric body and greater curvature at the level of tracheal carina and the gastroesophageal junction at the level of gastric fundus (lower gastric body). In addition, it presented a marked delay in the elimination of contrast through the pylorus. We did not identify the left hemidiaphragm. Then it was decided to request a chest computed tomography, which confirmed the findings. It was proposed surgical repair of large mixed hernia with possible risk of volvulus, but the patient refused surgery. He is currently asymptomatic.
Discussion
The repair of sliding hiatal hernias is indicated only in case of large hernias that cause symptoms of GERD refractory to medical treatment. By contrast, hiatal hernia types II, III and IV should be repaired early, even in the absence of symptoms, because of the risk of potentially serious complications such as volvulus of the stomach (1-3). In our case, the patient repeatedly refused surgical treatment and remains asymptomatic.
References
1. Pagán Pomar A, Palma Zamora E, Ochogavia Segui A, Llabres Rosello M. Laparoscopic surgery into mixed hiatal hernia. Results pre-operative and post-operative. Rev Esp Enferm Dig 2009;101:623-30. [ Links ]
2. Al-Balas H, Bani Hani M, Omari HZ. Radiological features of acute gastric volvulus in adult patients. Clinical Imaging 2010;34:344-7. [ Links ]
3. Shivanand G, Seema S, Srivastava DN, Pande GK, Sahni P, Prasad R, et al. Gastric volvulus: Acute and chronic presentation. Clinical Imaging 2003;27:265-8. [ Links ]

