










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.103 n.7 Madrid Jul. 2011
https://dx.doi.org/10.4321/S1130-01082011000700015
LETTERS TO THE EDITOR
Synchronic gastric adenocarcinoma and lymphoma
Adenocarcinoma y linfoma gástricos sincrónicos
Key words: Synchronic gastric neoplasia. Gastric adenocarcinoma. Gastric lymphoma.
Palabras clave: Neoplasia sincrónica gástrica. Cáncer gástrico. Linfoma gástrico.
Dear Editor,
The presence of multiple carcinomas in the stomach has been widely described in medical literature; however, much less common is the synchronic detection of gastric adenocarcinoma together with primary gastric lymphoma. Recently, the association between these synchronic tumours has been related to infection by Helicobacter pylori (1).
We present a new case in which an advanced gastric cancer is found synchronically with a gastric lymphoma.
Clinical case
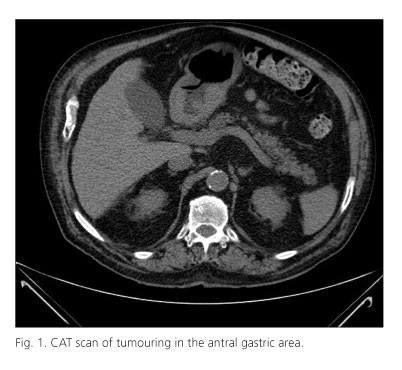
A 81 year old male with a clinical history of arterial hypertension, diabetes mellitus, chronic renal insufficiency and peripheral arteriopathy. He presents with toxic syndrome and gastric dyspepsia. An endoscopic study shows neo-formation at juxtapyloric antral level within the normal range which hinders the passage of the endoscope and prevents the exploration from continuing. The biopsy reports the presence of an adenocarcinoma. The analysis highlights hypochromic anaemia and some tumoral markers within the normal range (CEA: 3.17 µg/L, CA 19.9: 17.31 KU/L). An abdominal CT scan shows the formation of gastric tumors that extend along the entire lesser curvature to the duodenal bulb and the first part of the duodenum with adenopathies next to the inferior margin. Cholelithiasis. The patient does not present with retroperitoneal adenopathies or distance metastasis (Fig. 1). Surgical intervention shows antral neoplasia extended to the gastric body. Cholecystectomy, total gastrectomy and Roux-en-Y oesophageal-jejunostomy were also carried out. Anatomopathological study reports two neoplasic masses, with an ulcerous-necrotic centre and mamelonated margins, separated by 3 cm of normal-looking gastric wall. The nearest tumoral area measures 65 x 55 mm and features diffuse neoplasic proliferation which infiltrates the gastric wall and reaches the surrounding adipose tissue, and which is a high grade non-Hodgkin's lymphoma, compatible with a diffuse large B-cell lymphoma. The distal tumoral area measures 55 x 55 mm and features diffuse and glandular neoplasic proliferation made up of polygonal cells with an irregular round nucleus with a prominent nucleolus and broad, eosinophilic cytoplasm. The neoplasic proliferation infiltrates the gastric wall up to the muscular layer, without reaching the serous membrane or the adipose tissue. This is a diffuse, intestinal adenocarcinoma. Surgical resection margins are unaffected. Neoplasic infiltration through the adenocarcinoma is found in one of the 32 dried ganglia, without extracapsular extension. The patient has no post-operative complications. After assessing the patient, the oncological committee rejected adjuvant treatment because of the patient's commorbidities. The patient is monitored as an out-patient and showed good progress after 6 months.
Discussion
The synchronic presence of adenocarcinoma and gastric lymphoma was described for the first time by Rabinovitch in 1952 (2). Since then, 56 cases have been published in the medical literature (1,3).
The changes in the mucous surrounding the primary gastric lymphoma together with similar findings in the adenocarcinoma suggest that these two tumours could come from the same immunological dysfunction or share a common pathogenesis (4). It is believed that H. pylori contributes to the development of both the carcinoma and the lymphoma. The development of the adenocarcinoma is described by the H. pylori infection sequence and constitutes a chronic gastritis which predisposes the patient to intestinal metaplasia, which becomes dysplasia and then carcinoma. H. pylori causes lymphoid aggregates to appear in the submucous, after which the monoclonal proliferation of B cells in this lymphoid tissue can cause the appearance of a gastric MALT lymphoma (5-7). Furthermore, the tendency to present with secondary neoplasias has been suggested, in immunodepressed patients, as a possible explanation why the presence of gastric lymphoma seems to increase the risk of gastric carcinoma but not the other way round, which would also explain the small size of the adenocarcinoma in our patient.
These two entities present similar macroscopic characteristics in the endoscopic study and can lead to confusion, such as the diagnosis of multifocal lesions in the lymphoma. For this reason, a biopsy of all the suspected areas is recommended. Although there are no clinical guidelines for the treatment of synchronic gastric tumours, it is thought that treatment should follow the therapeutic guidelines for adenocarcinoma which involve total gastrectomy and D1 or D2 dissection (1). The treatment of choice for aggressive gastric lymphomas is chemotherapy which in our case has not been possible because of the patient's commorbidities.
Carles Olona-Casas, Vicente Vicente-Guillén, Aleidis Caro-Tarragó, Jose Ma Coronas-Riba and Enric Duque-Guilera
Department of General and Digestive Surgery. Hospital Universitario Joan XXIII. Tarragona, Spain
References
1. Hamaloglu E, Topalogu S, Ozdemir A, Ozenc A. Synchoronous and metachronous occurrence of gastric adenocarcinoma and gastric lymphoma: A review of the literature. World J Gastroenterol 2006;12 (22):3564-74. [ Links ]
2. Rabinovitch J, Pines B, Grayzel D. Coexisting lymphosarcoma and ulcer-carcinoma of the stomach. Arch Surg 1952;64:185-91. [ Links ]
3. Lee JH, Bae JS, Ryu KW, Lee JS, Park SR, Kim ChG, et al. Gastric cancer patients at high-risk of having synchronous cancer. World J Gastroenterol 2006;12(16):2588-92. [ Links ]
4. Zamboni G, Franzin G, Scarpa A, Bonetti F, Pea M, Mairuzzi GM, et al. Carcinoma-like signet-ring cells in gastric mucosa-associated lymphoid tissue (MALT) lymphoma. Am J Surg Pathol 1996;20:588-98. [ Links ]
5. Ishihama T, Kondo H, Saito D, Yamaguchi H, Kuniaki S, Yokota T, et al. Clinicopatholigical studies on coexisting gastric malignant lymphoma and gastric adenocarcinoma: report of four cases and review of the Japanese literature. Jpn J Clin Oncol 1997;27(2):101-6. [ Links ]
6. Kaffes A, Hughes L, Hollinshead J, Katelaris P. Synchronous primary adenocarcinoma, mucosa-associated lymphoid tissue lymphoma and a stromal tumor in a Helicobacter pylori-infected stomach. Journal of Gastroenterology and Hepatology 2002;17:1033-6. [ Links ]
7. Chan A, Chu K, Yuen S, Leung S, Lam S, Wong J. Synchronous gastric adenocarcinoma and mucosa-associated lymphoid tissue lymphoma in association with helicobacter pylori infection: comparing reported cases between the East and West. Am J Gastroenterol 2001; 96:1922-4. [ Links ]

