










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.103 no.12 Madrid dic. 2011
https://dx.doi.org/10.4321/S1130-01082011001200007
PICTURES IN DIGESTIVE PATHOLOGY
Iatrogenic esophageal perforation sealed by means of a self-expanding metal stent
Cierre de una perforación esofágica yatrogénica con una prótesis metálica autoexpandible
Jesús García-Cano, Cristina Jimeno-Ayllón and María Julia Morillas-Ariño
Department of Digestive Diseases. Hospital Virgen de la Luz. Cuenca, Spain
Case Report
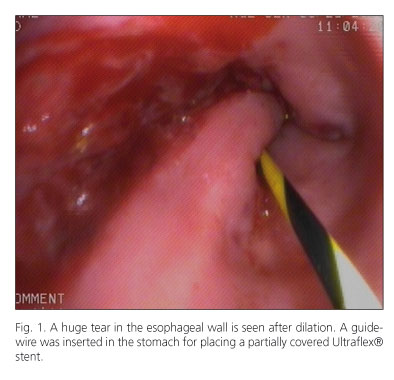
An 87-year-old man suffering from hiatal hernia and a Schatsky ring was coming to our unit for 15 years for regular dilations with Maloney dilators. In the last procedure, several minutes after dilation, the patient complained of chest pain. An upper endoscopy was performed. A huge tear in the left lateral side of the lower esophagus was seen (Fig. 1). Immediately, in that moment, insertion of a coated self-expanding stent was deemed to be the most appropriate measure. The gastroscope was advanced until the second duodenal portion and a superstiff guidewire was passed through the working channel of the endoscope. The gastroscope was withdrawn and a 10 cm long esophageal Ultraflex®, partially covered, was inserted with only endoscopic monitoring (1). The patient was admitted with n.p.o. and fluidotherapy. Four hours later, a CT thoracic scan was performed. No free air was seen in the mediatinum and the stent was in correct position.
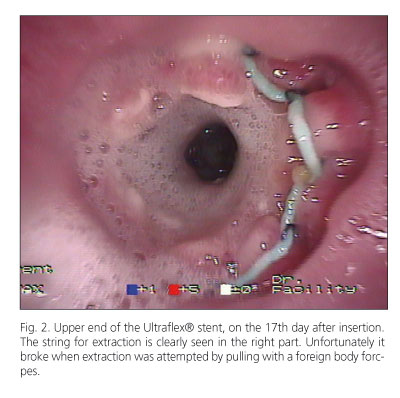
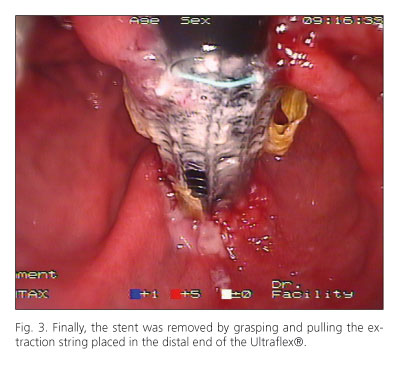
Only mild chest discomfort was noted. The patient began to eat a clear diet 48 hours after the procedure. The stent was removed 17 days later, grasping and pulling the string located in its upper end (Fig. 2). Unfortunately, the string was broken. Afterwards, the extraction manoeuvre succeeded grasping a similar string located in the distal end of the stent (Fig. 3). The patient did well.
Discussion
Removable esophageal stents have proven to be useful for healing esophageal perforations and leaks (2). The sooner the esophageal tear is sealed, the greatest the likelihood of an uneventful recovery for the patient. Besides, modern esophageal stents are easy to insert and many of them can be removed safely in a few weeks. After a dilation procedure, if there are serious concerns about a perforation has occurred, perhaps it is appropriate the immediately insertion of a covered removable esophageal stent to seal the possible perforation.
Maloney dilators have no an inner orifice to be slide over a guidewire like, for instance, Savary dilators. However, Maloney-type dilators are still used nowadays not only for physician controlled dilation but also for patient self-dilations in chronic benign esophageal strictures (3).
References
1. García-Cano J. Endoscopic insertion of oesophageal stents without fluoroscopic guidance. Scand J Gastroenterol 2005;40:1132-3. [ Links ]
2. Gelbmann CM, Ratiu NL, Rath HC, Rogler G, Lock G, Schölmerich J, et al. Use of self-expandable plastic stents for the treatment of esophageal perforations and symptomatic anastomotic leaks. Endoscopy 2004; 36:695-9. [ Links ]
3. Dzeletovic I, Fleischer DE, Crowell MD, Kim HJ, Harris LA, Burdick GE. Self dilation as a treatment for resistant benign esophageal strictures: outcome, technique and quality of life assessment. Gastrointest Endosc 2010;71:AB179. [ Links ]

