










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.104 n.2 Madrid Feb. 2012
https://dx.doi.org/10.4321/S1130-01082012000200017
LETTERS TO THE EDITOR
Giant fibrovascular esophageal tumor. Endoscopic vision
Pólipo fibrovascular gigante esofágico. Visión endoscópica
Key words: Giant esophageal polyp. Fibrovascular esophageal polyp. Endoscopic image of an esophageal polyp.
Palabras clave: Pólipo esofágico gigante. Pólipo fibrovascular esofágico. Imagen endoscópica de un pólipo esofágico.
Dear Editor,
The fibrovascular esophageal polyp is a rare, benign intraluminal tumor, also known as an inflammatory pseudotumor. The tumor consists of a mixture of inflamed fibrous and granulomatous tissues, along with lipomatous elements covered by a normal squamous epithelium (1).
Very few cases of giant (over 17 cm) fibrovascular esophageal polyps have been reported so far (2), and even less endoscopic images of them.
Case report
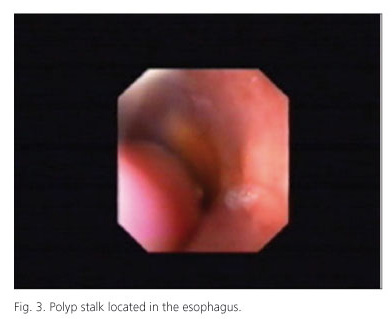
A 58-year-old man with a family history of type II diabetes mellitus and arterial hypertension, admitted with otalgia spreading to the neck and a high fever. The physical examination was normal. Analytically, VSG was 124. Reactive C protein: 14 and leukocytic. Laryngoscopy, Rx of thorax and computer tomography (TAC) of the ears were normal. Thoracic TAC showed an intraluminal esophageal mass of 16 x 7 cm arising from the cervical of the esophagus settling in the cardiac orifice of the stomach. Endoscopy: a large stalk of a polyp appeared, sprouting from below the Killian´s area, occupying practically 1/3 of the esophagus, running the length of the esophagus and ending in a circular polypoid mass of 7 cm, located in a small hiatus hernia. The histopathological study was negative for neoplastic cells, and a fibrovascular polyp was suspected.
The patient continued complaining dysphagia, thoracic pain and a sensation of a mass that came to the mouth. A left-cervical esophagotomy was performed to extract the polyp. Later, an anatomopathological study confirmed the diagnostic of a fibrovascular polyp. The patient presents no recurring symptoms or reappearances after follow up visits.


Discussion
The fibrovascular esophageal polyp normally forms in the part of the esophagus next to the cricopharyngeus muscle (3). They represent between 0.5 and 1% of non-epithelial benign esophageal tumors. Their occurrence is very rare. Clinically speaking, dysphagia is the most common symptom, although regurgitations, odynophagia, anorexia, gastrointestinal bledeeng produced by polyp ulceration, and asphyxiation caused by regurgitated polyp impacting the larynx (4), can all also be related to fibrovascular esophageal polyps.
In these patients, the diagnosis is usually made by endoscopy, barium swallow tests and/or TAC. The recurrence of these polyps is rare.
The treatment of these lesions is surgical excision. The exact location, size, pedicle thickness, and vascularization of the polyp will all determine the best method to apply: endoscopic or surgical (5).
Bartolomé García-Pérez1, Rocío García-Paredes2, Akiko Ono-Ono1, Manuel Miras-López1,
José Antonio Pons-Miñano1 and Luis Fernando Carballo-Álvarez1
1Service of Digestive Diseases. Hospital Universitario Virgen de la Arrixaca. Murcia, Spain.
2Section of Digestive Diseases. Complejo Hospitalario La Mancha-Centro. Alcazar de San Juan. Ciudad Real, Spain
References
1. Li Volsi VA, Perzin KH. Inflammatory pseudotumors (inflammatory fibrous polyps) of the esophagus. A clinicopathologyc study. Am J Dig Dis 1975;20: 475-81. [ Links ]
2. Solito B, Anselmino M, Tognetti A, Vignati S, Rossi M. Rare case of inflammatory fibrous polyp of the esophagus. Dis Esophagus 2002;15: 328-9. [ Links ]
3. SchuhmacherC, Becker K, Ditter H. Fibrovascular esophageal polyp as diagnostic challenge. Disease nof the Esophagus 2000;13:324-7. [ Links ]
4. Koyuncu M, Tekat A, Sesent T. Giant polyopid tumor of the esophagus. Auris Nasus Larynx 2000;27:363-6. [ Links ]
5. Zhang J, HaoHY, Li SWH, Zhang ST. Successful endoscopic removal of a giant upper esophageal inflammatory fibrous polyp. World J Gastroenterol 2009;15:5236-8. [ Links ]

