










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.104 n.4 Madrid Apr. 2012
https://dx.doi.org/10.4321/S1130-01082012000400011
LETTERS TO THE EDITOR
Splenic rupture following diagnostic colonoscopy
Ruptura esplénica tras colonoscopia diagnóstica
Key words: Splenic rupture. Endoscopy.
Palabras clave: Ruptura esplénica. Endoscopia.
Dear Editor,
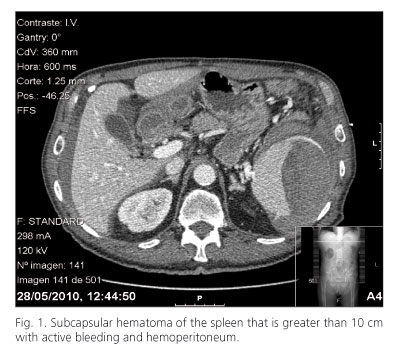
Male of 67 years of age with a history of ischemic heart disease and bypass graft aorto-biliac currently being treated with clopidogrel, atenolol, isosorbide mononitrate, and statins, who underwent colonoscopy because of general syndrome and anemia. A colonoscopy was performed with sedation medication administered (midazolam 4 mg and fentanyl 0.05 mg) and without complications to report, showing only internal hemorrhoids. Two hours later and after ensuring full recovery, the patient was discharged. Eight hours after the discharge, the patient experienced abdominal pain and sixteen hours later the patient suffered a presyncope episode and was transferred to an emergency department. A blood analysis showed that the patient presented anemia (9.5 g/dL hemoglobin) and an abdominal CT scan (Fig. 1) displayed a subcapsular hematoma of the spleen that was over 10 cm with active bleeding and hemoperitoneum. As the patient presents hemodynamic instability an emergency laparotomy with splenectomy and ligation of vessels was performed. Presence of 2 liter hemoperitoneum without intestinal perforation was confirmed during surgery. After the operation the patient made a satisfactory recovery and was discharged seven days later.
Discussion
Colonoscopies are a safe and routinely performed diagnostic and therapeutic procedure for different colorectal diseases, and most common complications include bleeding (1%) and perforation (0.1-0.2%) (1). Splenic rupture is a rare complication with less than eighty cases reported in the literature. With the increased number of colonoscopies, with particular reference to screening colorectal cancer, we must take into account that complications are rare but potentially fatal, and as the present case, that is characterized by abdominal pain left upper quadrant or scapula, progressive anemia and hypovolemic shock. Symptomatology typically begins in the first twenty four hours, but there are cases deferred until ten days. It is necessary a high index of suspicion to establish the diagnosis and CT scan is the indicated test. The main etiopathogenic factor postulated is the excessive traction on the spleno-colic ligament (2) in patients with previous abdominal surgery, and a way to minimize this complication could be to place the patient in left lateral decubitus when you go through the splenic flexure, because so spleen and flexure splenic do lower and it can decrease the traction on the adhesions (3). The treatment of choice is urgent laparotomy and splenectomy (4). Splenic embolization and conservative treatment are also possible in selected cases.
Roberto González-Soler, Elena Castro-Ortiz, Ángeles Lancho-Seco, Covadonga García-Suárez,
Eva Santos-Blanco, David Carral-Martínez, Susana Ávila-Nasi, Abel González-Ramírez and Leopoldo López-Rosés
Servicio de Aparato Digestivo. Hospital Xeral-Calde. Lugo, Spain
References
1. Macrae FA, Tan KG, Williams CB. Towards safer colonoscopy: a report on the complications of 5000 diagnostic or therapeutic colonoscopies. Gut 1983;24:376-83. [ Links ]
2. Espinal EA, Hoak T, Porter JA, Slezak FA. Splenic rupture from colonoscopy: a report of two cases and review of the literature. Surg Endosc 1997;11:71-3. [ Links ]
3. Tse CC, Chung KM, Hwang JS. Prevention of splenic injury during colonoscopy by positioning of the patient. Endoscopy 1998;30:S74-5. [ Links ]
4. Lalor PF, Mann BD. Splenic rupture after colonoscopy. JSLS. 2007;11:151-6. [ Links ]

