










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.104 no.5 Madrid may. 2012
https://dx.doi.org/10.4321/S1130-01082012000500007
PICTURES IN DIGESTIVE PATHOLOGY
Giant hepatocellular carcinoma
Carcinoma hepatocelular gigante
Paloma Álvarez Martínez1, Pablo Granero-Castro2, Iván Fernández-Vega3, Alfredo Renilla-González4, Luis Rodrigo-Sáez1 and María Varela-Calvo5
Departments of 1Gastroenterology, 2General Surgery, 3Pathology, 4Cardiology, and 6Gastroenterology and Hepatology. Liver Unit. Hospital Universitario Central de Asturias. Oviedo, Spain
Case report
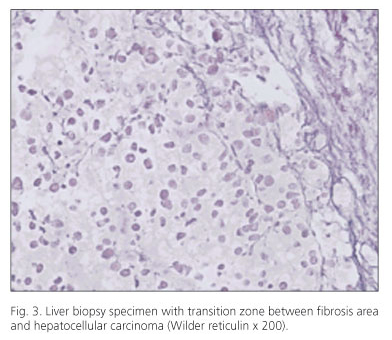
A 59-year-old man was admitted to the hospital because of an abdominal mass. The patient drank more than 60 g ethanol/day. He had no history of cirrhosis or other medical disorders. Physical examination revealed a cachectic appearance and a large, hard, non-tender abdominal mass occupying the right upper quadrant and epigastric area with a rich collateral circulation (Fig. 1). Laboratory data revealed alkaline phosphatase 189 IU/L; AST 59 IU/L; ALT 16 IU/L; GGT 83 IU/L; total serum bilirubin 1.96 mg/dL, alpha fetoprotein 87.6 ng/mL. Hepatitis B and C virus serology were negative. A computed tomography (CT) scan (Fig. 2) demonstrated a mass that measured 20 x 17 cm in diameter in the left lobe of the liver. Numerous tortuous vessels, infiltration of the inferior cava vein, and superior mesenteric vein thrombosis were also recognized. The splenic and portal veins were permeable. A final diagnosis of a moderately differentiated hepatocellular carcinoma (HCC) in a cirrhotic liver was established by fine needle aspiration cytology (Fig. 3). Due to end-stage of patient (ECOG performace status 3) best supportive care was the only treatment indicated. The patient died two months after diagnosis.


Discussion
A patient with cirrhosis and HCC detected at an end-stage (BCLC-D) is presented. More than 80% of HCC affect cirrhotic patients. Therefore, a strategy of 6-month surveillance with ultrasound would favor an early diagnosis in the asymptomatic phase of disease. A treatment with curative intention is possible during this clinical period, which would carry with it a 5-year survival higher than 80% (1,2).
Currently in Spain, more than 40% of HCC are detected casually or by symptoms associated with disease. This fact indicates the need to increase the identification of high-risk patients, who should be introduced into screening programs (3).
References
1. Bruix J, Sherman M. Management of hepatocellular carcinoma. Hepatology 2005; 42:1208-36. Updated Hepatology 2011. [ Links ]
2. El-Serag HB. Hepatocellular Carcinoma. N Engl J Med 2011;365:1118-27. [ Links ]
3. Varela M, Reig M, de la Mata M, Matilla A, Bustamante J, Pascual S. et al. Treatment approach of hepatocellular carcinoma in Spain. Analysis of 705 patients from 62 centers. Med Clin (Barc) 2010;134:569-76. [ Links ]

