










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.104 n.6 Madrid Jun. 2012
https://dx.doi.org/10.4321/S1130-01082012000600005
Endoscopic evaluation and histological findings in graft-versus-host disease
Evaluación endoscópica y hallazgos histológicos en la enfermedad de injerto contra huésped
Antonio Velasco-Guardado1, Lucía López-Corral2, Alberto Álvarez-Delgado1, Teresa Flores-Corral3, Fernando Geijo-Martínez1, Dolores Caballero-Barrigón2 and Antonio Rodríguez-Pérez1
Departments of 1Gastroenterology, 2Hematology, and 3Pathology. Hospital Universitario de Salamanca. Salamanca, Spain
ABSTRACT
Background: the gastrointestinal (GI) tract is the major target site of the graft-versus-host disease (GVHD). Diagnosis is based on endoscopic and histological findings.
Material and methods: we performed a retrospective study from January 1st, 1990 to December 31st, 2008 on 338 upper gastrointestinal endoscopies (gastroscopies) performed to 197 patients that underwent an allogeneic transplant with clinical suspicion of GI-GVHD.
Results: endoscopic findings to the diagnosis of GVHD have a sensitivity (S) of 34%, specificity levels (SP) of 65%, a positive predictive value (PPV) of 73% and a negative predictive value (NPV) of 48%. The histological study of the endoscopic biopsies has a global sensibility of 85.6% SP = 34.6% PPV = 64.2% and NPV = 63.7%. Histological grade was correlated with the clinical grade of acute GVHD (p = 0.018).
Conclusion: upper gastrointestinal endoscopy is useful for the diagnosis of GVHD, as it allows biopsies that can ultimately lead to the diagnosis, but with limited accuracy because the histological findings have low sensitivity and specificity, while the endoscopic findings are generally nonspecific.
Key words: Graft versus host disease (GVHD). Endoscopy. Histology.
RESUMEN
Introducción: el tracto gastrointestinal es la diana principal de afectación en la enfermedad de injerto contra huésped (EICH). Su diagnóstico se basa en los hallazgos endoscópicos e histológicos.
Material y métodos: hemos realizado un estudio retrospectivo, desde el 1 de enero de 1990 hasta el 30 de diciembre de 2008, de 338 endoscopias digestivas altas realizadas a 197 pacientes sometidos a trasplante alogénico de células hematopoyéticas con sospecha de EICH gastrointestinal.
Resultados: los hallazgos endoscópicos tienen una sensibilidad (S) del 34%, especificidad (E) del 65%, valor predictivo positivo (VPP) del 73% y valor predictivo negativo (VPN) del 48% para el diagnóstico de EICH. El estudio histológico de las biopsias tiene una S del 85,6%, E del 34,6%, VPP del 64,2% y VPN del 63,7%. El grado histológico se correlacionó con el grado clínico en la EICH aguda (p = 0,0018).
Conclusión: la endoscopia digestiva alta es útil para el diagnóstico de EICH, ya que permite la toma de biopsias que finalmente pueden llevar al diagnóstico, pero con una rentabilidad limitada ya que los hallazgos histológicos tienen una sensibilidad y especificidad bajas, mientras que los endoscópicos son generalmente inespecíficos.
Palabras clave: Enfermedad de injerto contra huésped (EICH). Endoscopia. Histología.
Introduction
Allogeneic stem cell transplant is the election treatment in patients with haematological malignant diseases. Activity has increased in the last years manly due to the higher age of patients (up to 65 years), as well as to the existence of a higher number of unrelated donors (> 13 millions); moreover, cord blood is now considered a suitable source of stem cells for adult patients. Graft-versus-host disease (GVHD) is the most important complication after allogeneic transplant and is associated with morbidity and mortality (1). Gastrointestinal acute GVHD presents as nausea, anorexia, vomiting, diarrhea, abdominal pain, hemorrhage and ileus and carries a > 80% risk of mortality in severe forms (grade III-IV) and do not respond to first line therapy (2). Acute GVHD is defined when it appears during the first 100 days (3).
Chronic GVHD appears after 100 days and is the most common cause of death other than disease after hematopoietic stem cell transplantation (HSCT) in this period (4). Prior acute GVHD is the most important risk factor for developing chronic GVHD (5).
Due to the frequency of gastrointestinal symptoms during the first 100 days after HSCT more than 50% of the patients will be referred for an endoscopic evaluation of the enteric tract. Differential diagnosis between GVHD and other conditions such as toxicity from chemotherapy or radiotherapy, drug-related side-effects, bacterial, viral, parasitical or fungal infections should be performed (6,7). Endoscopic findings in stomach and duodenum examinations in GVHD may vary between normal mucosa and several unspecific signs such as edema, erythema, frank ulcers and erosion of the mucosa (8).
Histological findings, regardless of the biopsied area, include apoptosis of crypt epithelial cells, destruction of the crypts and variable infiltration of lymphocytes in the epithelium and the lamina propria (6,9). In view of the endoscopic findings, the unspecific symptoms of the patients and the significant side-effects of the immunosuppressants used in GVHD therapy, a histological confirmation is required before starting with the treatment (10,11).
Early detection and definitive diagnosis of GVHD are essentials for successful treatment as it can help prevent irreversible organ damage and improve survival.
Unfortunately, the diagnosis of GVHD can be difficult to establish because of the nonspecific nature of associated symptoms, and it requires excluding other diagnoses such as infection, drug effects, malignancies and residual post-inflammatory damage and usually causes a diagnostic challenge to the hematologist. That is the reason why involvement of multidisciplinary team, including gastroenterologists, is critical.
Material and methods
We performed a retrospective study in all the patients who received an allogeneic HSCT in the University Hospital of Salamanca from January 1, 1990 to December 31, 2008, and who were referred to our Department for an upper gastrointestinal endoscopy due to GVHD suspicion. The endoscopic findings of these explorations were retrospectively compiled, as well as the histological findings of the biopsies (three biopsies at least) performed during the procedure. The stain used was standard hematoxylin and eosin. The presence of apoptotic bodies in the biopsy specimen (minimum criterion), crypt abscesses, and/or destruction of glands were considered criteria for a diagnosis of acute or chronic GVHD, after ruling out other causes that also could induce these findings, such as drug-related toxicity or infections by blood and/or stool cultures, cytomegalovirus infection by antigenemia assay, or a reduced dose of the suspect drug.
Endoscopic findings have been gradually staged according to the classification proposed by Cruz-Correa (12) (Fig. 1): stage 0: normal; stage I: loss of vascular pattern and/or focal moderate erythema; stage II: edema and/or diffuse moderate erythema; stage III: edema, erythema, erosions and/or bleeding; stage IV: ulceration, exudates and/or bleeding.

In the histological analysis, the presence of apoptotic bodies was considered to be "compatible with GVHD". The histological findings have been gradually staged according to the classification proposed by McDonald and Sales (13) in 1984: grade 0: normal; grade I: single cell necrosis (apoptosis) noted on medium power; grade II: evidence of epithelial damage by crypt/glandular abscesses, epithelial flattening or glandular/crypt dilation; grade III: dropout of one or more crypts/glands, grade IV: total epithelial denudation.
In the descriptive analysis of the sample, percentages were used for qualitative variables, and measures of central tendency (mean and/or median if there was great asymmetry or dispersion) and dispersion (standard deviation) for quantitative variables. We used SPSS v. 15.0 (Chicago, Illinois, USA) for those calculations. All dichotomous variables were analyzed with χ2 test in contingency tables in order to compare the distribution of categorical variables, as well as Fisher's exact test and Monte Carlo simulations. A 95% confidence interval for the odds ratio was used, and the continuous and categorical variables were analyzed with ANOVA test and we used the Pearson's r correlation coefficient.
Results
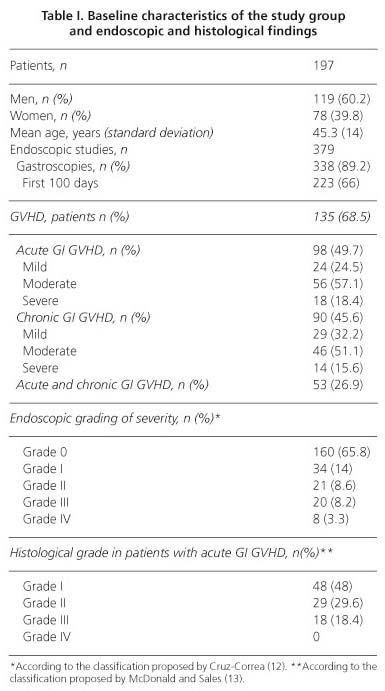
Baseline characteristics of the study group and endoscopic and histological findings are summarized in table I.
Endoscopic diagnosis of GVHD
Three hundred thirty eight endoscopies of the upper gastrointestinal tract were performed in 197 patients with suspect diagnosis of acute or chronic GVHD; macroscopic endoscopic data compatible with GVHD were present in only 83 patients with GVHD (34.2%). On the other hand, in patients without histological and clinical confirmation of GVHD, the 35.3% (n = 30) showed an endoscopy compatible with GVHD. Endoscopic findings to the diagnosis of GVHD have a sensitivity (S) of 34%, specificity levels (SP) of 65%, a positive predictive value (PPV) of 73% and a negative predictive value (NPV) of 48%.
Endoscopic findings in patients with GVHD according to the classification of endoscopic severity -Cruz-Correa (12) classification- were not related with clinical severity.
Histology
Biopsy was performed in 331 out of the 338 upper endoscopies (98%). The esophagus was biopsied in 19 explorations (7.8%), the stomach in 324 (92.2%) and the duodenum in 18 (7.4%). Stomach biopsies had a sensitivity of 89%, specificity of 30.6%, PPV of 63.8%, and NPV of 67%. In the esophagus, S = 33.3%, SP = 100%, PPV = 100%, and NPV = 41%, and in duodenum S = 80%, SP = 62.5%, PPV = 57%, and NPV = 83.3%. When all locations were united, S = 85.6% SP = 34.6% PPV = 64.2%, and NPV = 63.7%.
Histological severity was significantly associated with clinical severity (p = 0.018) with a Pearson's r correlation of 0.24 (p = 0.006).
Histological severity was not related to the endoscopic findings -according to the Cruz-Correa (12) classification-.
Complications
Digestive bleeding after the biopsy has been registered as a complication, with an incidence of 2% (n = 4). In three of these cases, they were mild, and in one case, it was moderate bleeding which required endoscopic techniques in order to be controlled.
Discussion
GVHD and endoscopy
Gut GVHD is a frequent complication after allogeneic SCT; more than 50% of the patients will be sent to the endoscopic room in order to confirm this clinical diagnosis. Although histological confirmation is needed to establish the diagnosis, macroscopic diagnosis is crucial in order to begin the treatment on the day of the endoscopy.
Our results shows that diagnostic based only on endoscopic findings is poor, with a high percentage of false positives and negatives and it were not related to the clinical severity of GVHD. In a retrospective study in which patients with GVHD suspect underwent gastroscopy and biopsy (11), no differences were found with regard to the endoscopic findings or the symptoms among the patients that were later diagnosed with gastrointestinal GVHD and those who were not diagnosed with that condition. In this study, 18% of the patients with histological results compatible with GVHD presented normal endoscopic results.
The best gastrointestinal site to take a biopsy is unknown (14). The most logical approach would be to take a biopsy of a certain area according to the predominant symptoms (15). Thomson et al. (14) carried out a prospective study with 24 patients in 2006, in which they combined gastroscopy (taking gastric and duodenal biopsies), colonoscopy (biopsies of left and right colon) and ileoscopy (biopsy of terminal ileum) in transplanted patients who suffered diarrhea over the first 100 days after the transplant. They obtained a higher diagnostic yield with biopsies of the left colon (82%), compared with 77% in biopsies of the right colon, 68% in the ileum, 65% in the duodenum and 71% in the antrum. The combination of colonoscopy plus ileoscopy and colonoscopy plus gastroscopy showed the highest percentages of positive biopsies (95 and 94%, respectively).
In 2008, Ross et al. conducted a prospective study with 112 patients who simultaneously underwent a biopsy of the stomach, the duodenum and the rectosigmoid colon for the diagnosis of gastrointestinal GVHD and obtained that rectosigmoid biopsies revealed the highest levels of diagnostic yield for GVHD with regard to sensitivity, specificity, PPV and NPV, compared with all other locations (95.6, 100, 100 and 84%, respectively). The sensitivity of gastric and duodenal biopsies was 72.5% (p < 0.00001) and 79.2% (p = 0.0018), respectively, while NPV was 45.6% for the stomach (p = 0.0039) and 52.5% (p = 0.02) for the duodenum (7). Our results are similar to these, with a global sensitivity of 85.6%, but with a low NPV (63.7%).
GVHD and histology
The anatomopathological interpretation of stages I and II in the postoperative period is not without difficulties (16). First of all, the histological changes secondary to pre-transplant therapy for cyto-reduction may imitate GVHD. These changes that are secondary to a drug-related toxicity usually take place over the first 20 days after transplantation, although there have been described cases after the 30st day (17,18). Infections in the post-transplantation period (bacterial, fungal, parasitic and viral) are also a problem, because they can produce signs and symptoms that are similar to GVHD, especially cytomegalovirus infections (19).
Cheung et al. (20) published a retrospective study in 2008 in which they compared the endoscopic findings and the histological ones from 101 patients. The endoscopic findings revealed a significantly positive statistical relation with histological abnormalities (OR = 33.6; 95% CI: 4.3-261.1).
In 1994, a study found a gradual difference from 0 to 1 between the histological and the endoscopic (macroscopic) classifications of acute GVHD in 87.6% of endoscopies (21). However, a more recent study (14) found a difference from 2 to 4 stages in 28.2% of biopsies compared with the endoscopic assessment. In this study, a histological diagnosis of acute GVHD was obtained in 44.7% of the biopsies of endoscopically normal areas, which highlights the need of performing biopsies in areas with seemingly normal mucosa. These authors consider that the histopathological stage is not useful in the assessment of the severity of GVHD in transplanted patients, and they assert that the predictive factors for response and mortality in GVHD should be established after the clinical severity criteria. In our study, 65.8% of patients with GVHD had a normal endoscopy.
On the other hand, a recent study with 27 patients with GVHD (determined via colon biopsies) has shown that histological stages III and IV, compared with stages I and II, do not only present more intense symptoms (p = 0.01), but also require second-line treatments due to corticoid refractoriness (p = 0.027), and they present a higher mortality associated to GVHD complications (p = 0.05) (22). These data are compatible with our results, because we obtain a positive correlation between histological stages and clinical severity (Pearson's r = 0.24; p = 0.006), but fail to achieve this correlation with endoscopic involvement.
We conclude that upper endoscopy is useful for the diagnosis of GVHD, allowing the taking of biopsies that can ultimately lead to the diagnosis, but with limited accuracy because the histological findings have low sensitivity and specificity, while the endoscopic findings are usually nonspecific. It is necessary to perform biopsies of apparently normal mucosa areas because a high percentage of histological diagnosis is obtained.
References
1. Welniak LA, Blazar BR, Murphy WJ. Immunobiology of allogeneic hematopoietic stem cell transplantation. Annu Rev Immunol 2007;25:139-70. [ Links ]
2. Leisenring WM, Martin PJ, Petersdorf EW, Regan AE, Aboulhosn N, Stern JM, et al. An acute graft-versus-host disease activity index to predict survival after hematopoietic cell transplantation with myeloablative conditioning regimens. Blood 2006;108:749-55. [ Links ]
3. Ferrara JL, Levine JE, Reddy P, Holler E. Graft-versus-host disease. Lancet 2009;373:1550-61. [ Links ]
4. Lee SJ, Klein JP, Barrett AJ, Ringden O, Antin JH, Cahn JY, et al. Severity of chronic graft-versus-host disease: association with treatment-related mortality and relapse. Blood 2002;100:406-14. [ Links ]
5. Carlens S, Ringden O, Remberger M, Lonnqvist B, Hagglund H, Klaesson S, et al. Risk factors for chronic graft-versus-host disease after bone marrow transplantation: a retrospective single centre analysis. Bone Marrow Transplant 1998;22:755-61. [ Links ]
6. Cox GJ, Matsui SM, Lo RS, Hinds M, Bowden RA, Hackman RC, et al. Etiology and outcome of diarrhea after marrow transplantation: a prospective study. Gastroenterology 1994;107:1398-407. [ Links ]
7. Ross WA, Ghosh S, Dekovich AA, Liu S, Ayers GD, Cleary KR, et al. Endoscopic biopsy diagnosis of acute gastrointestinal graft-versus-host disease: rectosigmoid biopsies are more sensitive than upper gastrointestinal biopsies. Am J Gastroenterol 2008;103:982-9. [ Links ]
8. Fallows G, Rubinger M, Bernstein CN. Does gastroenterology consultation change management of patients receiving hematopoietic stem cell transplantation? Bone Marrow Transplant 2001;28:289-94. [ Links ]
9. Ponec RJ, Hackman RC, McDonald GB. Endoscopic and histologic diagnosis of intestinal graft-versus-host disease after marrow transplantation. Gastrointest Endosc 1999;49:612-21. [ Links ]
10. Bombi JA, Nadal A, Carreras E, Ramirez J, Munoz J, Rozman C, et al. Assessment of histopathologic changes in the colonic biopsy in acute graft-versus-host disease. Am J Clin Pathol 1995;103:690-5. [ Links ]
11. Roy J, Snover D, Weisdorf S, Mulvahill A, Filipovich A, Weisdorf D. Simultaneous upper and lower endoscopic biopsy in the diagnosis of intestinal graft-versus-host disease. Transplantation 1991;51:642-6. [ Links ]
12. Cruz-Correa M, Poonawala A, Abraham SC, Wu TT, Zahurak M, Vogelsang G, et al. Endoscopic findings predict the histologic diagnosis in gastrointestinal graft-versus-host disease. Endoscopy 2002;34:808-13. [ Links ]
13. McDonald GB, Sale GE. The human gastrointestinal tract after allogeneic marrow transplantation. In: Sale GI,Shulman HM, editors. The Pathology of Bone Marrow Transplantation. New York: Masson; 1984. p. 83. [ Links ]
14. Thompson B, Salzman D, Steinhauer J, Lazenby AJ, Wilcox CM. Prospective endoscopic evaluation for gastrointestinal graft-versus-host disease: determination of the best diagnostic approach. Bone Marrow Transplant 2006;38:371-6. [ Links ]
15. Vogelsang GB, Lee L, Bensen-Kennedy DM. Pathogenesis and treatment of graft-versus-host disease after bone marrow transplant. Annu Rev Med 2003;54:29-52. [ Links ]
16. Nguyen CV, Kastenberg DM, Choudhary C, Katz LC, DiMarino A, Palazzo JP. Is single-cell apoptosis sufficient for the diagnosis of graft-versus-host disease in the colon? Dig Dis Sci 2008;53:747-56. [ Links ]
17. Sloane JP, Norton J. The pathology of bone marrow transplantation. Histopathology 1993;22:201-9. [ Links ]
18. Snover DC. Graft-versus-host disease of the gastrointestinal tract. Am J Surg Pathol 1990;14(Supl.1):101-8. [ Links ]
19. Snover DC. Mucosal damage simulating acute graft-versus-host reaction in cytomegalovirus colitis. Transplantation 1985;39:669-70. [ Links ]
20. Cheung DY, Kim JI, Kim SS, Sung HY, Cho SH, Park SH, et al. Endoscopic evaluation in gastrointestinal graft-versus-host disease: comparisons with histological findings. Dig Dis Sci 2008;53:2947-54. [ Links ]
21. Kreisel W, Fauser AA, Dolken G, Herbst EW. Gastroenterologische Befunde bei Graft-Versus-Host-Disease (GVHD) nach Allogener Knochenmarktransplantation. Z Gastroenterol 1991;29:289-93. [ Links ]
22. Melson J, Jakate S, Fung H, Arai S, Keshavarzian A. Crypt loss is a marker of clinical severity of acute gastrointestinal graft-versus-host disease. Am J Hematol 2007;82:881-6. [ Links ]
![]() Correspondence:
Correspondence:
Antonio Velasco-Guardado
Department of Gastroenterology
Hospital Universitario de Salamanca
Paseo San Vicente, 50-180
37007 Salamanca, Spain
e-mail: antoniovelascog@usal.es
Received: 23-12-2011
Accepted: 10-04-2012

