










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.104 no.7 Madrid jul. 2012
https://dx.doi.org/10.4321/S1130-01082012000700011
LETTERS TO THE EDITOR
Megaesophagus and emetic syndrome as first clinical manifestations of scleroderma
Megaesófago y síndrome emético como primera manifestación clínica de una esclerodermia
Key words: Systemic sclerosis. Scleroderma. Esophageal dilatation. Gastroesophageal reflux.
Palabras clave: Esclerosis sistémica. Esclerodermia. Dilatación esofágica. Reflujo esofágico.
Dear Editor,
Esophageal involvement in scleroderma is a common complication characterized by motility alterations and gastroesophageal reflux. We report the case of a patient presenting with megaesophagus associated with scleroderma diagnosed after an incidental radiologic finding.
Case report
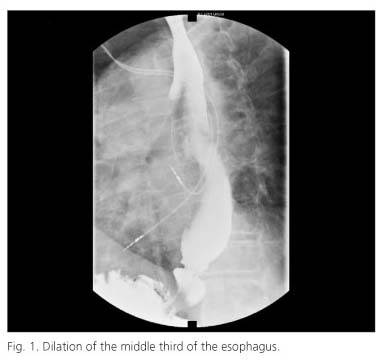
A 68-year-old male patient with a previous history of small-bowel diverticulosis and chronic airflow obstruction followed up in the Neumology Service. A thoracic CT scan revealed significant dilation of the middle and distal third of the esophagus, dilated esophagus at the level of the gastric cardias with hydroaereal level in the middle third. The patient was referred to the Digestive Department. The patient also complained of pyrosis and nocturnal irritative cough of several years of evolution. The physical examination showed the presence of malar teleangiectasias. Biochemistry revealed a discrete normocytic anemia and elevated C-reactive protein. During his follow-up period, the patient suffered from several episodes of hematic content vomiting. Several endoscopies were carried out showing marked esophageal dilation, a permanently open cardiac sphincter and erosive lesions in the esophageal mucosa compatible with reflux esophagitis. Three months later, the patient presented with pseudo-occlusive symptoms which required surgery. The operation discarded mechanical obstruction. The esophagus/gastroduodenal study with barium showed hypotonic and dilated esophagus (Fig. 1) as well as marked duodenal and small bowel dilation (Fig. 2). The patient did not tolerate esophageal manometry test and the functional study was completed with isotopic esophageal scintigraphy which revealed severe transit delay compatible with adynamia of the esophageal body and presence of severe gastroesophageal reflux. Antitransglutaminase antibodies IgA, ANA, anti-DNA, AML, ANCA were negative. Anti-centromere antibody determination yielded positive results (1:320).

In a new interview with the patient, he complained of clinical symptoms compatible with Raynaud's phenomenon affecting the fingers of both hands after exposure to cold during the last three years. The patient was then referred to the Collagen-related Disorders Unit where a capillarosocopy and the analysis of the previous information confirmed the diagnosis of scleroderma.
Discussion
Scleroderma is a multisystemic autoimmune disease which involves the gastrointestinal tract in 82% of patients. Esophageal affectation reaches 90% although the presence of megaesophagus is rare. The motility pattern shows hypocontractile esophageal body and lower esophageal sphincter hypotony, which favours gastroesophageal reflux and associated complications.
Our patient presented with an esophageal motility pattern compatible with scleroderma, but it could not be confirmed by means of manometry. The suspected scleroderma was confirmed in the Collagen-related Disorders Unit of our institution.
The pseudo-occlusive symptoms affecting our patient appear in at least 10% of the patients and imply severe intestinal involvement and lower survival rates.
We must bear in mind that esophageal body adynamia together with lower esophageal sphincter hypotony prompt us to discard scleroderma and we want to remark the role of isotopic esophageal scintigraphy in the diagnosis of the esophageal motility pattern whenever manometric studies are not available or are not tolerated by the patient.
Ángela Araujo-Míguez, Ángeles Pizarro-Moreno, Francisco Bellido-Muñoz and Marta Garzón-Benavides
Hospital Universitario Virgen del Rocío. Seville, Spain
References
1. Forbes A, Marie I. Gastrointestinal complications: the most frequent internal complications of systemic sclerosis. Rheumatology 2009; 48(Supl. 3):36-9. [ Links ]
2. Martínez Caselles A, Martínez Pascual C, Moreno Martínez MJ, Sánchez Torres A, Carballo Álvarez LF. Hemorragia por telangiectasias en paciente con esclerosis sistémica. Rev Esp Enferm Dig 2011; 103:326-7. [ Links ]
3. Wielosz E, Borys O, ychowska I, Majdan M. Gastrointestinal involvement in patients with systemic sclerosis. Pol Arch Med Wewn. 2010;120:132-6. [ Links ]
4. Ebert EC. Esophageal disease in scleroderma. J Clin Gastroenterol 2006;40:769-75. [ Links ]
5. Ntoumazios SK, Voulgari PV, Potsis K, Koutis E, Tsifetaki N, Assimakopoulos DM. Esophageal involvement in scleroderma: gastroesophageal reflux, the common problem. Semin Arthritis Rheum 2006; 36:173-81. [ Links ]

