










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.104 no.7 Madrid jul. 2012
https://dx.doi.org/10.4321/S1130-01082012000700012
LETTERS TO THE EDITOR
Iliac-appendiceal fistula. An unusual cause of gastrointestinal bleeding
Fístula iliaco-apendicular. Una causa inusual de hemorragia digestiva
Key words: Iliac-appendiceal fistula. Aortoenteric fistula. Gastrointestinal bleeding.
Palabras clave: Fístula iliaco-apendicular. Fístula aortoentérica. Hemorragia digestiva.
Dear Editor,
Aortoenteric fistula (AEF) defined as a communication between the aorta and the wall of the intestinal tract is a rare cause of gastrointestinal bleeding, which is associated with a high death rate and calls for high clinical suspicion in the diagnosis and an urgent surgical response.
We report on the case of a patient with a primary iliac-appendiceal fistula, presenting symptoms of lower gastrointestinal bleeding.
Case report
A 59 year old woman who came to the Emergency Department with massive, painless rectal bleeding, fever and syncope. Her personal history showed the following: epidermoid carcinoma of the cervix operated on in 2004 (hysterectomy, double adnexectomy, radiotherapy and brachytherapy), epidermoid carcinoma of the tongue in 2005 and atypical posterior pulmonary resection from metastasis.
Upon entry, she was in a stable condition, with hemoglobin levels of 7.8 g/dL and a hematocrit of 24%. The simple X-ray of the abdomen and the abdominal ultrasound were non-specific. Endoscopic investigations showed remains of blood in the colon, without identifying the cause. An abdominal computerized axial tomography (CT scan) revealed a gaseous collection at the level of the right iliopsoas (Fig. 1).

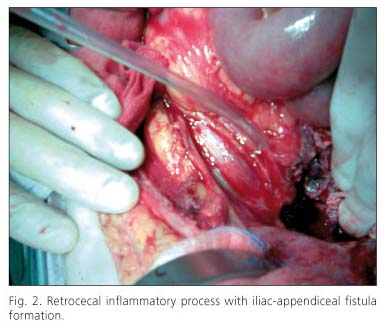
In the light of these findings and the continued rectal bleeding an operation was performed on the patient on the fourth day after admission, in the form of an emergency laparotomy (Fig. 2) during which a retrocecal inflammatory process was found affecting cecum, appendix and encompassing the right iliac artery, and confirming the existence of Iliac-appendiceal fistula formation. An extended right hemicolectomy and a femoro-femoral saphenous vein bypass were carried out. The patient made good progress, and was released 14 days after the operation.
Pathological anatomy reported a section of the right hemicolectomy with mucous necrosis and a significant amount of blood material in part organized in the appendiceal bed. This study displayed metastatic foci of squamous cell carcinoma affecting the serosa, fatty tissue and perineural and perivascular regions (great vessels). Isolated lymph nodes with no evidence of malignancy and endoarterial material with groups of squamous tumour cells were also found.
Discussion
Most AEF cases are secondary to previous aorta surgery (1). Primary fistulas are not common and are usually associated with arteriosclerosis aneurysms (90%), radiotherapy, injury trauma, neoplasms, pancreatic pseudocysts, ulcer disease, diverticulitis, appendicitis and arterial infections (2,3).
The part of the gastrointestinal tract most frequently at risk of developing a fistula is the duodenum (80%), especially the 3rd portion (3). Our case is unusual because of the location and cause of the fistula. We are talking about Iliac-appendiceal fistula formation caused by neoplastic relapse at the level of the great vessels and right colon. The extreme mobility of the appendix makes it susceptible to becoming involved in any intra-abdominal pathology (4,5). Tyson et al. published details of a case of iliac-appendiceal fistula in 1969 (6).
The main clinical sign is gastrointestinal bleeding, which is usually intermittent and sometimes very slight or bloodless at the beginning, and which is the main cause of death among these patients (2).
It is a very serious problem and accurate diagnosis requires a high degree of clinical suspicion. Endoscopy and CT scan are the diagnostic techniques most widely used, although not infrequently these techniques give negative results (2,3), with most cases being diagnosed by means of an exploratory laparotomy (as in the case we have discussed) which should be carried out as soon as clinical suspicions are aroused, because the mortality rate without surgical treatment is close to 100% (1).
Inmaculada Monjero-Ares1, Carlos Gegúndez-Gómez1, Francisco Javier Rielo-Arias2, Ana Elisa Álvarez-Gutiérrez1,
Juan Pena-Holguín2, Marlén Alvite-Canosa1, Rocío González-López1, Eva Iglesias-Porto1, María Isabel Pérez-Moreiras1 and Félix Arija-Val1
1Department of General and Digestive Surgery. 2Department of Vascular Surgery. Hospital Universitario Lucus Augusti. Lugo, Spain
References
1. Morales Ruiz J, Selfa Muñoz A, Salmerón Escobar J. Hipovolemic shock caused by an aortoenteric fistula: an unusual cause of gastrointestinal bleeding. Gastroenterol Hepatol 2011;34:586-7. [ Links ]
2. Riera Vázquez R, Manuel-Rimbau Muñoz E, Julia Montoya J, Cordobés Gual J, Merino Mairal O, Lara Hernández R, et al. Primary aortoenteric fistula: a rare cause of gastrointestinal bleeding in young adults. Gastroenterol Hepatol 2005;28:26-9. [ Links ]
3. Acosta A, Karatanasopuloz Pintos R, Haydar C, Levy G, Martín C, Paiz M. Aortoenteric fistula as cause of digestive bleeding in three adult patients. Med Intensiva 2006;30:120-2. [ Links ]
4. Fievé G, Bour P. Aortoappendicular fistula after aortoiliac prosthetic replacement. Ann Vasc Surg 1989;3:187-9. [ Links ]
5. Matsuura K, Takahara Y, Sudo Y, Ishida K, Nakajima N. A Case of Fistula of the Right Iliac Aneurism to the Appendix. Ann Vasc Surg 2002;16:768-70. [ Links ]
6. Kitzmiller JW, Robb HJ, Barkel D, Clift D, Klein S, Madrazo A. Iliac appendiceal fistula: Case presentation and review of management. J Vasc Surg 1984;1:696-6. [ Links ]

