










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.104 no.7 Madrid jul. 2012
https://dx.doi.org/10.4321/S1130-01082012000700016
LETTERS TO THE EDITOR
Acute appendicitis by Enterobius vermicularis, an unusual etiology in children
Apendicitis aguda por Enterobius vermicularis, una etiología inusual en niños
Key words: Enterobius vermicularis. Acute appendicitis. Children.
Palabras clave: Enterobius vermicularis. Apendicitis aguda. Niños.
Dear Editor,
The Enterobius vermicularis (EV) is one of the most common gastrointestinal helminth infections in children. Acute appendicitis (AA) is the most prevalent surgical emergency in pediatrics. The role of worms in the development of histologically confirmed AA is controversial, although the obstruction of the appendicular lumen could act as an exceptional trigger.
Case report
A 7-year-old boy went to emergency department with severe abdominal pain of 20 hours, located in the right iliac fossa. Fever. Alimentary vomit. Normal bowel movements.
On examination, the child had general status affectation. Abdominal palpation aimed to voluntary defense in FID. Blumberg and psoas signs were positive.
Laboratory tests showed leukocytosis with neutrophilia and eosinophilia. Ultrasound visualized retrocaecal appendix of 6 mm.
Urgent laparotomy appendectomy was performed, appreciating macroscopic inflammation of the appendix, without free liquid. Normal ileum.
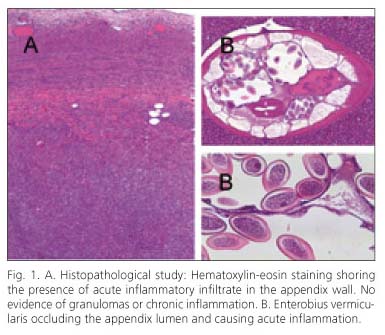
Histopathological examination confirmed the diagnosis of appendicitis; cells of acute inflammation were invading the wall (Fig. 1A) and pinworms occluding the lumen (Fig. 1B).
Given these findings, we contacted the family to start treatment with mebendazole.
Discussion
The AA is the most common surgical cause of abdominal pain in children. It may be triggered by obstruction, decreased blood flow, mucosal ischemic injury or bacterial infection. Parasitic infections represent a minimum percentage of causes (2,3). The fecaliths are the most common trigger, but some parasites may be involved in its formation (4).
The presence of EV in the context of an AA ranges from 0.2 to 3.8% (5). Helminthic invasion originates appendicular cramps caused by intermittent luminal obstruction, simulating a picture of AA (6). Courses of perianal itching, bruxism and insomnia may also be present. The histopathological study shows infiltration of the appendicular wall by neutrophils and eosinophils, with granulomas and necrosis. In exceptional cases, obstruction of the appendicular lumen by EV causes appendicitis confirmed histologically with acute inflammation (7).
The diagnosis of appendicitis is clinical. Laboratory tests, radiography and abdominal ultrasound are additional tests, but not diagnostic. In the context of a clinical appendicitis, the presence of previous appendicular colic and eosinophilia should make us to consider the existence of concomitant parasitic infection. Moreover, In the presence of perianal pruritus, bruxism and insomnia we must suspect the appendicular colonization by EV (8,9).
Face with a clinical diagnosis of AA, emergency appendectomy is indicated. Laparoscopic appendectomy is associated with an increased risk of intraperitoneal settlement in the case of gastrointestinal helminthic infection (9). Laparotomy appendectomy is considered a safer technique.
The systematic review of the histopathological examination of the appendices has demonstrated the incidental presence of parasites, being EV the most prevalent in children (10). Their discovery allows starting the treatment of the patient and family with mebendazole to eradicate the parasitic infection.
In conclusion, the systematic review and histological study of the appendages is essential. The incidental finding of intestinal parasitism by EV permits to start anthelminthic treatment. Performing an exhaustive medical history will help to identify clinical and laboratory data indicative of parasitic infection.
Yolanda Martínez-Criado, Ana Millán-López, Nicoleta Galán and Juan Carlos de-Agustín-Asensio
Department of Pediatric Surgery. Hospital infantil Virgen del Rocío. Seville, Spain
References
1. Mowlavi GH, Massoud J, Mobedi I, Rezaian M, Solaymani Mohammadi S. Enterobius vermicularis: a controversial cause of appendicitis. Iran J Publ Health 2004;33:27e-31. [ Links ]
2. Sidky HA, Maksoud MA, Aziz HA, Saleh A. Acute appendicitis as a complication of helminthic infection among some Egyptian patients. J Egypt Soc Parasitol 1981;11:469-73. [ Links ]
3. Feng CS. Parasites in faecaliths. J Clin Pathol 1988;41:232-3. [ Links ]
4. Grimes C, Chin D, Bailey C, Gergely S, Harris AM. Appendiceal faecaliths are associated with right iliac fossa pain. Ann R Coll Surg Engl 2010;92:61e4. [ Links ]
5. Sah SP, Bhadani PP. Enterobius vermicularis causing symptoms of appendicitis in Nepal. Trop Doct 2006;36:160-2. [ Links ]
6. Wiebe BM. Appendicitis and Enterobius vermicularis. Scand J Gastroenterol 1991;26:336-8. [ Links ]
7. Aydin O. Incidental parasitic infestations in surgically removed appendices: a retrospective analysis. Diagnostic Pathology 2007;2:16. [ Links ]
8. Arca MJ, Gates RL, Groner JI, Hammond S, Caniano DA. Clinical manifestations of appendiceal pinworms in children: an institutional experience and a review of the literature. Pediatr Surg Int 2004;20:372-5. [ Links ]
9. Saxena AK, Springer A, Tsokas J, Willital GH. Laparoscopic appendectomy in children with Enterobius vermicularis. Surg Laparosc Endosc Percutan Tech 2001;11:284e6. [ Links ]
10. Nemeth L, Reen DJ, O'Briain DS, McDermott M, Puri P. Evidence of an inflammatory pathologic condition in "normal" appendices following emergency appendectomy. Arch Pathol Lab Med 2001;125:759e64. [ Links ]

