










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.105 no.1 Madrid ene. 2013
https://dx.doi.org/10.4321/S1130-01082013000100015
LETTERS TO THE EDITOR
Tenofovir treatment of the severe acute hepatitis B
Tratamiento con tenofovir de la hepatitis aguda B de evolución grave
Key words: Acute hepatitis. Hepatitis B virus. Jaundice.
Palabras clave: Hepatitis aguda. Virus hepatitis B. Ictericia.
Dear Editor,
The pharmacological treatment of the acute hepatitis B has become increasingly important over the last 10 years due to the fact that the infection is still an important public health problem and one of the main causes of acute liver failure in our environment. However, there are only a few studies about this subject and most of them are conducted with lamivudine with a low methodological quality (1-5). This is the reason why we submit this clinical case of severe acute hepatitis B treated with tenofovir which presented a good clinical evolution. The major clinical practice guidelines (6,7) currently recommend the antiviral treatment of severe acute hepatitis B, as it may reduce the mortality and the risk of acute liver failure in this kind of patients (5).
Case report
A fifty-five-year-old male, with no medical history, seeks medical consultation after five days of asthenia, hyporexia, jaundice of the skin and eyes, choleretic urine and hypocolic stools. In the urgent analysis, there is a strong presence of cytolisis (AST 1720 UI/dL, ALT 2660 UI/dL), hyperbilirubinemia (total bilirubin 20.94 mg/dL) and coagulopathy (prothrombin activity, 45%; INR, 1.79). HBV serologies turned out to be positive (HBsAg +, anti-HBc IgM + and AgHBe +). The serologies of the HCV, HDV and HIV turned out to be negative.
In the presence of severe acute liver failure, it is decided to use a specific treatment for the acute hepatitis B with tenofovir 245 mg/24 hours from the first day of the hospital admission.
The patient remained hospitalized for a period of 14 days, without having hepatic encephalopathy or any external signs of bleeding at any moment. The analytical figures started to improve from the day number 7 of the antiviral treatment. Subsequently, the patient continued the treatment with tenofovir as an outpatient, the anti-HBe seroconversion occurred one month after the treatment was started and the HBsAg loss 8 weeks after the treatment was started. After two consecutive serologies HBsAg negative and anti-HBs positive, the antiviral treatment was suspended.
Discussion
The existing bibliography related to the treatment of the acute hepatitis B is sparse and relatively recent. The first prospective document dates from the year 2004, when Schmilowitz-Weiss et al. (1) treated 15 patients with severe acute hepatitis (INR > 1.6, bilirubin > 10 mg/dL or hepatic encephalopathy), achieving a response rate of 86% (Table I). Subsequently, in the year 2007, we can find the first randomised clinical trial (3), which included a total of 71 patients with acute hepatitis B, from which 31 randomised to lamivudine for 3 months and 40 of them to placebo. The study did not show any statistically significant differences in any clinical or analytical parameter, not even in the subset of 47 patients with the diagnosis of severe hepatitis which the trial included.
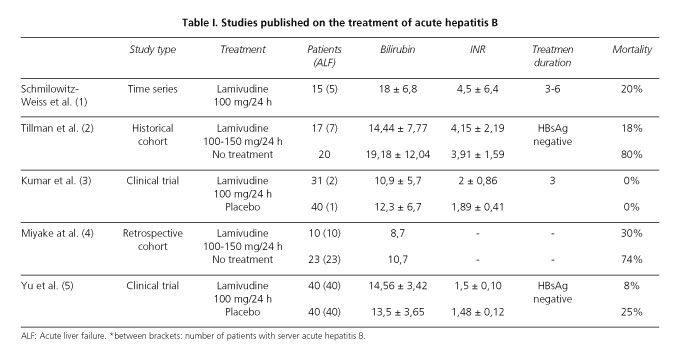
Finally, the most recent randomised clinical trial, conducted by Yu et al. (5) in the year 2010, included 80 patients, who were randomised to lamivudine and placebo, and that showed very promising results. The group who received lamivudine presented a lower mortality (7.5 vs. 25%) and a lower incidence of acute liver failure (20 vs. 42.5%). The study also showed that the sooner the treatment is initiated (the first 7 days), the better the clinical and analytical response rate of these patients.
Despite the mixed results of the literature, it is currently -recommended the pharmacological treatment of the severe acute hepatitis B (6,7), as it is observed the increase of patient survival rates and the decrease of the risk of acute liver failure in these patients. It is also recommended to start the treatment as soon as possible (5).
As for the drug of choice, despite the absence of studies with tenofovir or entecavir, the major clinical practice guidelines (6,7) recommend the use of the new antiviral drugs because of their high power and the absence of resistances. The duration of the treatment is not established, but the european guideline recommends the treatment for a period of at least 3 months after the seroconversion to anti-HBs (7).
Fernando Casals-Seoane, Beatriz Arberas-Díez and Luisa García-Buey
Department of Digestive Diseases. Hospital Universitario de La Princesa/Instituto de Investigación Sanitaria Princesa (IP).
Centro de Investigación Biomédica en Red de Enfermedades Hepáticas y Digestivas (CIBEREHD). Madrid, Spain
References
1. Schmilovitz-Weiss H, Ben-Ari Z, Sikuler E, Zuckerman E, Sbeit W, Ackerman Z, et al. Lamivudine treatment for acute severe hepatitis B: a pilot study. Liver Int 2004;24:547-51. [ Links ]
2. Tillmann HL, Hadem J, Leifeld L, Zachou K, Canbay A, Eisenbach C, et al. Safety and efficacy of lamivudine in patients with severe acute or fulminant hepatitis B, a multicenter experience. J Viral Hepat 2006;13:256-63. [ Links ]
3. Kumar M, Satapathy S, Monga R, Das K, Hissar S, Pande C, et al. A randomized controlled trial of lamivudine to treat acute hepatitis B. Hepatology 2007;45:97-101. [ Links ]
4. Miyake Y, Iwasaki Y, Takaki A, Fujioka S, Takaguchi K, Ikeda H, et al. Lamivudine treatment improves the prognosis of fulminant hepatitis B. Intern Med 2008;47:1293-9. [ Links ]
5. Yu JW, Sun LJ, Zhao YH, Kang P, Li SC. The study of efficacy of lamivudine in patients with severe acute hepatitis B. Dig Dis Sci 2010;55:775-83. [ Links ]
6. Lok AS, McMahon BJ. Chronic hepatitis B: update 2009. Hepatology 2009;50:661-2. [ Links ]
7. European Association for The Study Of The Liver. EASL Clinical Practice Guidelines: Management of chronic hepatitis B virus infection. J Hepatol (2012). Available at: http://dx.doi.org/10.1016/j.jhep.2012.02.010. [ Links ]

