










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versão impressa ISSN 1130-0108
Rev. esp. enferm. dig. vol.105 no.9 Madrid Out. 2013
https://dx.doi.org/10.4321/S1130-01082013000900013
LETTERS TO THE EDITOR
Endometrioid adenocarcinoma in the lower rectum
Adenocarcinoma endometroide de recto bajo
Key words: Endometriosis. Endometrioid adenocarcinoma. Rectal cancer. Rectorrhagia.
Palabras clave: Endometriosis. Adenocarcinoma endometroide. Cáncer de recto. Rectorragia.
Dear Editor,
Endometriosis is a common disease that usually involves the ovary (1) and generally has a benign course (2). Malignization is exceptional (fewer than 1%), affecting the rectum in only 5% of reported cases (2).
Case report
A 39-year-old woman with an uneventful history presents with abdominal pain in the left iliac fossa, weight loss, and rectorrhagia lasting 6 months. A mass effect is palpated 6 cm away from the anal margin during digital examination. CA125 is elevated (522.2 U/mL) whereas CEA and CA19-9 remains normal. Colonoscopy reveals friable mucosa at 7 cm from the anal margin, which suggests extrinsic compression and precludes echoendoscopy because of stenosis. Biopsies were negative for malignancy. An abdominal CT scan unveils a big, partially necrotized rectal growth, perirectal adenopathies, and uncertain uterus infiltration (Fig. 1). Finally, transvaginal ultrasound shows a vascularized solid mass, 65x56x68 mm in size, of likely digestive origin.

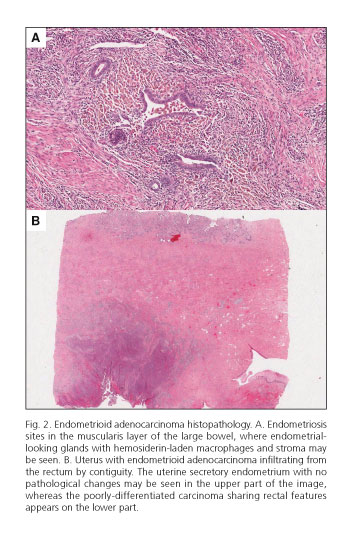
In the absence of a histological diagnosis an exploratory surgery is decided upon. Following the opening of the peritoneal reflection a tumour is observed in the mid-lower rectum, and a rectal anterior resection is performed. Histopathological examination documents a poorly-differentiated, infiltrating, endometrioid adenocarcinoma over endometriosis sites within the rectal muscularis layer with intestinal wall infiltration (Fig. 2A), nodal metastases, and a cytokeratin 7-positive and cytokeratin 20-negative immunohistochemical pattern with estrogen receptors positivity. In view of these results surgery is completed with hysterectomy and double annexectomy, and the presence of an endometrioid adenocarcinoma infiltrating the uterine wall from the rectum by contiguity is confirmed, with no endometriosis sites in the uterus (Fig. 2B).
The postoperative course was uneventful; the patient received adjuvant radio-chemotherapy following discharge and remains disease-free after one year.
Discussion
Fewer than 50 cases of intestinal tumours associated with endometriosis have been reported, with endometrioid adenocarcinoma being the commonest variant. Most cases occur in postmenopausal women receiving estrogen therapy following hysterectomy and double annexectomy for endometriosis. The clinical picture usually presents with abdominal pain, metrorrhagia and/or rectorrhagia (3). Tumours are usually found in the sigmoid colon, upper rectum, and rectovaginal septum, being exceptional in the extraperitoneal mid-lower rectum.
The etiopathogenesis is unknown, and in most cases endometriotic implants are secondary to retrograde menstruation (4). Hyperestrogenism is a potential risk factor (5), and genetic predisposition is suggested for cases without it (5). On the other hand, the neurological hypothesis described by Possover and Anaf (6,7) correlates endometriotic implants with sympathetic nervous system distribution; this might account for our patient's case since the mid-lower rectum's location is extraperitoneal and in intimate contact with the sympathetic plexus.
This case meets all the histological criteria defined by Sampson (8) for endometrioid adenocarcinoma, with tumour cells growing from endometriotic foci within the rectal muscularis coat, hence not from invasion from the uterus. Furthermore, the histology of the hysterectomy specimen confirms uterine infiltration by contiguity from the rectum, with no endometriotic sites in the uterus or annexes, and an endometrium with normal characteristics, which rules out a uterine origin.
There is no consensus protocol regarding the treatment of choice. At any rate, the need for radical resection of the involved intestinal segment plus hysterectomy and double annexectomy is indisputable. Adjuvant therapy is warranted by the presence of nodal metastases and uterine infiltration.
To conclude, endometrioid adenocarcinoma of the rectum is a rare tumour that requires a high index of suspicion for diagnosis. Importantly, it should be differentiated from colorectal tumours in order to optimize management and for its prognostic value. Our case is atypical in terms of age at presentation, absence of relevant history, and tumour location.
Yurena Caballero1, Ángel Turégano1, Eudaldo López-Tomassetti1,
María Soledad Martínez2, Virginia Benito3 and Juan Ramón Hernández1
Departments of 1General and Digestive Surgery, and 2Pathology.
Hospital Universitario Insular de Gran Canaria. Las Palmas de Gran Canaria, Spain.
3Department of Oncological Gynecology.
Hospital Universitario Materno Infantil de Gran Canaria. Las Palmas de Gran Canaria, Spain
References
1. Petersen VC, Underwood J, Wells M, Sheperd N. Primary endometroid adenocarcinoma of the large intestine arising in colorectal anastomosis. Histhopathology 2002;40:171-6. [ Links ]
2. Heaps JM, Nieberg RK, Berek JS. Malignant neoplasm arising in endometriosis. Obstet Gynecol 1990;75:1023-8. [ Links ]
3. Yantiss RK, Clement PB, Young RH. Neoplastic and pre-neoplastic changes in gastrointestinal endometriosis: A study of 17 cases. Am J Surg Pathol 2000;24:513-24. [ Links ]
4. Bouhmidi A, Sánchez Torres A, Martínez Jiménez T, Sáez Macia R, Sánchez de la Villa G, Montes Clavero C. Rectosigmoid endometriosis. Rev Esp Enferm Dig 2006;98:797-8. [ Links ]
5. Zanetta GM, Webb MJ, Li H, Keeney GL. Hyperestrogenism: A relevant risk factor for the development of cancer from endometriosis. Gynecol Oncol 2000;79:18-22. [ Links ]
6. Possover M, Rhiem K, Chiantera V. The "neurologic hypothesis": A new concept in the pathogenesis if the endometriosis? Gynecol Surgery 2005;2:107-11. [ Links ]
7. Anaf V, El Nakadi I, Simon P, Van de Stadt J, Fayt I, Simonart T, et al. Preferential infiltration of the large bowel endometriosis along the nerves of the colon. Hum Reprod 2004;19:996-1002. [ Links ]
8. Sampson JA. Endometrial carcinoma of the ovary arising in endometrial tissue in that organ. Arch Surg 1925;10:1-72. [ Links ]

