










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.106 n.3 Madrid Mar. 2014
LETTERS TO THE EDITOR
Development of a duodenal gallstone ileus with gastric outlet obstruction in a patient with a huge duodenal diverticulum
Desarrollo de un íleo duodenal y obstrucción gástrica por cálculo biliar en un paciente con un divertículo duodenal gigante
Key words: Bouveret syndrome. Gallstone ileus. Duodenal diverticulum. Gastric outlet obstruction.
Dear Editor,
A 66-year-old female complained of abdominal right upper quadrant pain, which persisted for 20 days. Then, she was admitted to our hospital with early satiety and repeated postprandial vomiting.
An esophago-gastro-duodenoscopy was performed, during which 1.2 L of gastric content was removed by endoscopic suction. A duodenal diverticulum leading into a cavity of 3 cm diameter was detected near the duodenal papilla and a big stone (about 3 cm in diameter) was impacted in the lumen of the second part of the duodenum (Fig. 1). Endoscopic extraction failed to remove the gallstone.
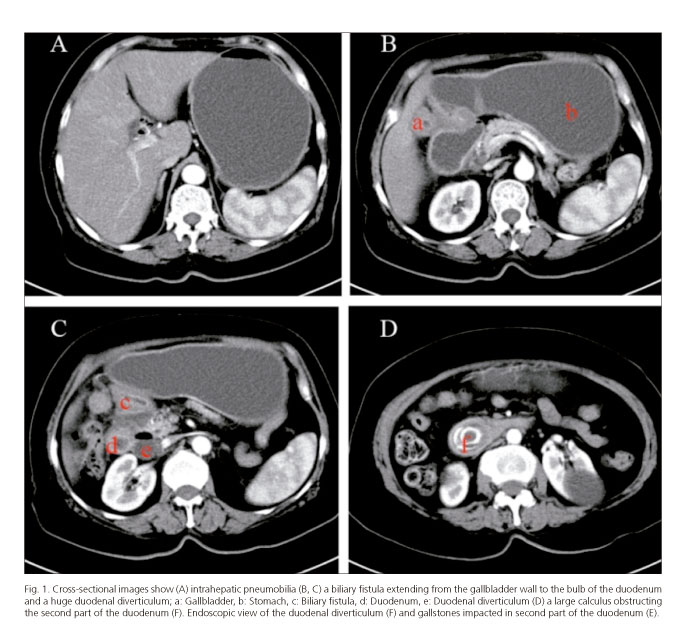
A CT scan of the abdomen (Fig. 1) revealed a gallstone ileus with a 7 × 3 cm gallstone in the second part of the duodenum, coexistence with a duodenal diverticulum and a fistula between the gallbladder and the duodenal bulb, as well as minimal pneumobilia.
The impacted gallstone was surgically removed by laparotomy and duodenotomy. Cholecystectomy and repair of the fistula was performed.
Discussion
Gallstone ileus is often a geriatric surgical emergency accounting for 1-3% of cases of mechanical intestinal obstruction (1), which occurs in 15 % of patients with a biliary enteric fistula. The majority of location for intestinal obstruction by a biliary calculus is the terminal ileum. Duodenal obstruction accounts for only 2 %-3 % of the cases (2). Bouveret syndrome is a rare complication of cholelithiasis in which calculi become impacted in the duodenum or pylorus, resulting in gastric outlet obstruction. It was first described by Leon Bouveret in 1896 and occurs most commonly in elderly women.
Duodenal diverticulum without severe complications does not require surgical intervention. In principle, for gallstone ileus, the primary therapeutic goal should be to relieve the gallstone obstruction and eventually repair the bilio-digestive fistula (3). Gallstones could be treated by endoscopy or surgery. Endoscopic extraction is less invasive, but it often fails when the obstructing calculus is very large. Furthermore, since gallstones that get impacted in the duodenum tend to be quite large, surgery is an optimal treatment. There are a one-stage approach with enterotomy, cholecystectomy and resection of the fistula at once, or a two-stage approach with an emergency enterotomy to remove the obstructing gallstone and cholecystectomy after a period of recuperation. Some reports have pointed out that the spontaneous closure of the biliary fistula following the passage of the stone, particularly when the cystic duct is patent and/or when there are no residual stones (4,5), therefore some authors questioned the need of repair of the biliary fistula (6). In our opinion, for clinically stable patients with comorbid diseases (such as diabetes mellitus, cerebrocardiovascular diseases), single-stage procedure should be advocated to avoid future risk of recurrent gallstone ileus, cholangitis and cholecystitis. Therefore, we performed a laparotomy with simultaneous extraction of the gallstone, cholecystectomy and repair of the fistula, though no retained gallstones in the patient was found.
Yong Zhou1, Xu-Dong Wu2, Ren-Gen Fan3, Hui-Min Ding4, Cheng-Lin Qin5 and Jing Jia6
Departments of 1,3,4,5General Surgery, 2Gastroenterology and 6Nephrology.
Yancheng city No. 1 people's hospital. Yancheng, China
References
1. Clavien PA, Richon J, Burgan S, Rohner A. Gallstone ileus. Br J Surg 1990;77:737-42. [ Links ]
2. Langhorst J, Schumacher B, Deselaers T, Neuhaus H. Successful endoscopic therapy of a gastric outlet obstruction due to gallstone with intracorporeal laser lithotripsy: a case of Bouveret's syndrome. Gastrointest Endosc 2000;51:209-13. [ Links ]
3. Palomeque-Jiménez A, Calzado-Baeza S, Reyes-Moreno M. Bouveret syndrome: an infrequent presentation of gallstone ileus. Rev Esp Enferm Dig 2012;104:324-5. [ Links ]
4. Shioi Y, Kawamura S, Kanno K, Nishinari Y, Ikeda K, Noro A, et al. A case of gallstone ileus displaying spontaneous closure of cholecystoduodenal fistula after enterolithotomy. Int J Surg Case Rep 2012;3:12-5. [ Links ]
5. Lobo DN, Jobling JC, Balfour TW. Gallstone ileus: Diagnostic pitfalls and therapeutic successes. J Clin Gastroenterol 2000;30:72-6. [ Links ]
6. O'Neill C, Colquhoun P, Schlachta CM, Etemad-Rezai R, Jayaraman S. Gastric outlet obstruction secondary to biliary calculi: 2 cases of Bouveret syndrome. Can J Surg 2009;52:E16-8. [ Links ]

