










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versão impressa ISSN 1130-0108
Rev. esp. enferm. dig. vol.106 no.5 Madrid Mai. 2014
LETTERS TO THE EDITOR
Retroperitoneal hematoma in Crohn's disease patient with warfarin therapy
Hematoma retroperitoneal en varón joven con enfermedad de Crohn en tratamiento con warfarina
Key words: Crohn's disease. Warfarin. Retroperitoneal hematoma.
Palabras clave: Enfermedad de Crohn. Warfarina. Hematoma retroperitoneal.
Dear Editor,
We present the case of a 49-year-old male, with sulfa, penicillin and cephalosporin allergy, previously diagnosed with Crohn's disease at the age of 15, corticodependent, with azatiophrine therapy 150 mg per day, permanent ileostomy and on warfarin therapy for 6 years due to superior limb venous thrombosis event.
We followed him as outpatient in the Inflammatory Bowel Disease Unit. He complained of lethargy with a concomitant slightly decrease in the hemoglobin and hematocrit values. For that reason, he was started on oral iron therapy and low doses of oral corticosteroids because the patient also presented an increase in the frequency of ileostomy's drainage. Neither upper and lower endoscopies (through the ileostomy) nor videocapsule endoscopy revealed abnormalities. Although the abdominal scan showed at least two abscesses in the mesogastric area, one of 10cm in diameter and the other adjacent of 9cm, he did not refer abdominal pain, fever or leucocytes (Fig. 1A).
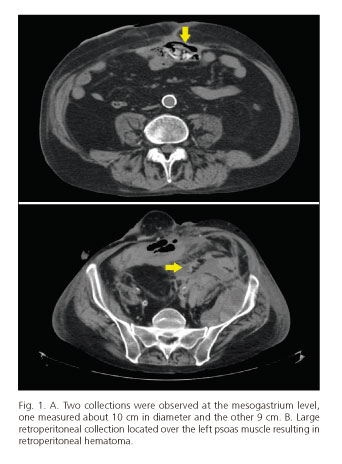
The patient was then started on empirical antibiotic therapy based on IV metronidazol and piperacilina/tazobactam. The abdominal magnetic resonance did not show different findings compared with previously abdominal tomography, but it demonstrated edema and periarticular fluid that produced an enlargement of the left coxofemoral articulation. The patient did not improve, and in the following days presented inguinal pain that radiated to the ipsilateral knee with a significantly functional impairment, back pain and mass sensation located on left flank associated with hypotension and tachycardia that went worse in a couple of hours. Blood analysis showed an elevated white cell count and a decrease in the hemoglobin value. Another abdominal tomography was urgently performed, and it showed a massive retroperitoneal hematoma (Fig. 1B).
We must state that our patient was on warfarin therapy for six years and 6 months before he was admitted to hospital and presented a fluctuation in his INR (international normalized ratio) value: 2,7, 1.6, 3.1 y 3.6. The patient was in hemodynamic shock so he underwent emergency surgery that showed that the retroperitoneal hematoma was due to the rupture of the psoas muscle. He entered the intensive care unit, where he was stabilized. His clinical, analytic and radiologic results improved, controlling the bleeding and the abdominal abscesses that were also drained.
Discussion
Crohn's disease is an inflammatory chronic entity that presents periods of flare and remission. It is well known that because of its transmural character, there are more predispositions to form fistulas and abdominal abscesses, and also to produce thrombotic phenomenon due to unknown mechanisms. In our case, the patient was on warfarin therapy because of the thrombotic events he presented in the past. Warfarin is an extensively used agent in the prophylaxis of thromboembolic events, and because of its many pharmacology interactions and its significant variability in its therapeutic ranges, it is always recommended its strict follow-up.
Our case is exceptional, because although there have been reports of retroperitoneal hematoma in anticoagulated patients (1-6), up to now no cases of Crohn's disease and retroperitoneal hematoma have been reported, in addition to an abdominal abscess formation, that we believe has enhanced and promoted retroperitoneal hemorrhage. On the other hand, as we know, corticosteroids are an essential tool in the treatment of chronic inflammatory diseases such as rheumatoid arthritis and inflammatory bowel disease, but we also know that their use is associated with multiple adverse effects. And in this sense some publications describe that warfarin interactions with other drugs increase the risk of bleeding. In fact, it has been postulated that steroids influence hepatic metabolism of warfarin, thereby increasing their availability, and thus, the risk of bleeding (7-9). As discussed before, there are reported cases of retroperitoneal hematoma secondary to rupture of the ilio-psoas muscle in anticoagulated patients, as our patient (3-5), and also it has been reported cases of retroperitoneal hematoma in anticoagulated patients receiving metronidazole and paracetamol (5,10), and we believe that because patients with inflammatory bowel disease need corticosteroid treatment on a regular basis as well as antibiotics, especially when they are with disease activity, we must emphasize the importance of studying these drug interactions that may not be taken into account in the context of a patient with poor outcome of his underlying disease as it is the case of the patient presented before, and therefore complex to treat.
In conclusion, we think it is important to notify this case, and insist in the necessity of using a more rigorous preventive strategy, with more thrombotic controls in patients with both inflammatory bowel disease and chronic anticoagulation, and even more cautious if they also are on corticoids or antibiotics therapy, because they are undoubtedly a high risk group for the development of complications.
Calixto Duarte-Chang, Luisa Castro-Laria, Federico Arguelles-Arias,
Ángel Caunedo-Álvarez and Juan Manuel Herrerías-Gutiérrez
UGC Digestive Disease. Hospital del Universitario Virgen Macarena. Sevilla, Spain
References
1. Sunga KL, Bellolio MF, Gilmore RM, Cabrera D. Spontaneous retroperitoneal hematoma: etiology, characteristics, management, and outcome. J Emerg Med 2012;43:e157-61. [ Links ]
2. Zago G, Appel-da-Silva MC, Danzmann LC. Iliopsoas muscle hematoma during treatment with warfarin. Arq Bras Cardiol 2010;94:e1-3. [ Links ]
3. Ozkan OF, Guner A, Cekic AB, Turan T, Kaya U, Reis E. Iliopsoas haematoma: A rare complication of warfarin therapy. J Coll Physicians Surg Pak 2012;22:673-4. [ Links ]
4. Murena L, Vulcano E, Salvato E, Marano M, D'Angelo F, Cherubino P. Bilateral iliopsoas intramuscular bleeding following anticoagulant therapy with heparin: A case report. Cases J 2009;2:7534. [ Links ]
5. Phillips S, Barr A, Wilson E, Rockall TA, Stebbing JF. Two cases of retroperitoneal haematoma caused by interaction between antibiotics and warfarin. Emerg Med J 2006;23:e8. [ Links ]
6. González C, Penado S, Llata L, Valero C, Riancho JA. The clinical spectrum of retroperitoneal hematoma in anticoagulated patients. Medicine (Baltimore) 2003;82:257-62. [ Links ]
7. Hromádková L, Interactions between glucocorticoids and warfarin in chronic inflammatory (autoimmune) diseases. Vl ek J.Vnitr Lek 2012;58:354-6. [ Links ]
8. Sellam J, Costedoat-Chalumeau N, Amoura Z, Aymard G, Choquet S, Trad S, et al. Potentiation of fluindione or warfarin by dexamethasone in multiple myeloma and AL amyloidosis. Joint Bone Spine 2007;74:446-52. [ Links ]
9. Stading JA, Chock A, Faulkner MA, Skrabal MZ. Effects of prednisone on the International Normalized Ratio. Am J Health Syst Pharm 2006;63:2354-6. [ Links ]
10. Andrews FJ. Retroperitoneal haematoma after paracetamol increased anticoagulation. Emerg Med J 2002;19:84-5. [ Links ]

