










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.106 no.6 Madrid jun. 2014
LETTERS TO THE EDITOR
Gallstone ileus and intestinal perforation secondary to sigmoid diverticulum
Íleo biliar con perforación secundaria de divertículo sigmoideo
Key words: Gallstone ileus. Intestinal oclusion. Diverticular stenosis. Diverticular perforation.
Palabras clave: Íleo biliar. Oclusión intestinal. Estenosis diverticular. Perforación de divertículo.
Dear Editor,
Biliary or gallstone ileus is a rare disease representing 1 % to 4 % of all mechanical intestinal obstruction cases. Gallstone impaction may be facilitated by changes in intestinal dynamics, prior inflammatory conditions, or both benign and malignant stenosing lesions. The most common site for impaction is the terminal ileum (60 %), whereas colonic obstruction is much less common, represents only 4.1 % of gallstone ileus cases (1,2), and is usually secondary to the passage of gallstones through a cholecystocolonic fistula with subsequent impaction in a previously diseased area (3). Surgical treatment is considered of choice, and single-stage procedures (enterotomy, fistula repair, and cholecystectomy) have a higher mortality rate despite they reduce the need for reintervention and/or complications from persistent biliodigestive fistula (1,4,5).
Case report
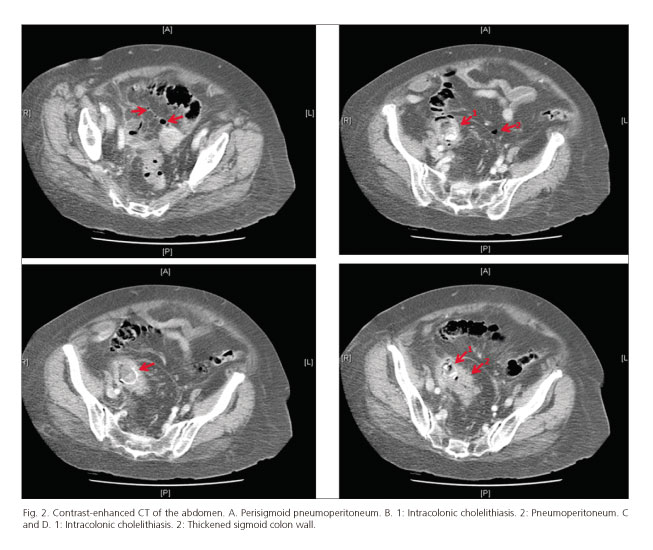
We report the case of an 84-year-old woman who presented at the emergency room with diffuse abdominal pain, more severe in the lower hemiabdomen, associated with vomiting and failure to pass gas and stools for 4 days. Her personal history included hypertension, dyslipidemia, and a procedure for ovarian cyst rupture at 15 years of age. The examination revealed moderate abdominal distension and diffuse abdominal tenderness with peritoneal irritation. Lab tests on admission showed leukocytosis at 11,700/mm3 and C-reactive protein over 90 mg/dl, with the remaining parameters within normal range. Abdominal X-rays showed findings consistent with intestinal obstruction at the descending-sigmoid colon. Abdominal computerized tomography (CT) revealed pneumobilia within the liver (Fig. 1), choledochus, and gallbladder walls with moderately dilated loops down to the sigmoid colon, where an intraluminal calcified nodule, 3 x 2 cm in size, could be seen with distal sigmoid wall thickening, multiple diverticula, perisigmoid extraluminal air bubbles, and a moderate amount of free fluid (Fig. 2), all this associated with biliary ileus, gallstones impacted in a sigmoid stricture and intestinal perforation. Surgery unveiled an inflammatory mass in the right hypochondrium, purulent peritonitis, sigmoid diverticular perforation prior to severe cholelithiasis, and thickened wall area in the sigmoid colon (Fig. 3). A sigmoidectomy procedure with terminal colostomy (Hartmann's technique) was performed, in accordance with the oncologic principles of resection for potential stenosis secondary to neoformation. Pathology documented the presence of inflammatory tissue with multiple diverticula and no malignant findings, all this associated with diverticular stenosis. The patient had a favorable outcome and was discharged on day 7 following the procedure. A second procedure was carried out for cholecystectomy, cholecystocolonic fistula repair, and transit restoration.


Fuensanta Mon-Martín, Alejandro Morales-Hernández,
Luciano J. Delgado-Plasencia and Antonio Alarcó-Hernández
Department of General Surgery. Hospital Universitario de Canarias.
La Laguna, Tenerife. Islas Canarias, Spain
References
1. Reisner RM, Cohen JR. Gallstone ileus: a review of 1001 reported cases. Am Surg 1994;60:441-6. [ Links ]
2. López Martínez C, Planells Roug M, García Espinosa R, Rodero Rodero. Íleo biliar. Aportación de nuestra casuística (21 casos). Cir Esp 1997;61:357-60. [ Links ]
3. Pérez Morera A, Pérez Díaz D, Calvo Serrano M, De Fuentemayor Valera ML, Martín Merino R, et al. Acute obstruction of the colon secondary to biliary lithiasis. Rev Esp Enferm Dig 1996;88:805-8. [ Links ]
4. Martínez Ramos D, Daroca José JM, Escrig Sos J, Paiva Coronel G, Alcalde Sánchez M, Salvador Sanchís JL. Gallstone ileus: management options and results on a series of 40 patients. Rev Esp Enferm Dig 2009;101:117-20,121-4. [ Links ]
5. Nakao A, Okamoto Y, Sunami M, Fujita T, Tsuji T. The oldest patient with gallstone ileus: Report of a case and review of 176 cases in Japan. Kurume Med J 2008;55:29-33. [ Links ]

