










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versão impressa ISSN 1130-0108
Rev. esp. enferm. dig. vol.106 no.8 Madrid Dez. 2014
Value of a step-up diagnosis plan: CRP and CT-scan to diagnose and manage postoperative complications after major abdominal surgery
Valor de una estrategia diagnóstica ascendente: CRP y CT en el diagnóstico y manejo postoperatorio de complicaciones tras cirugía abdominal importante
Jennifer Straatman1, Miguel A. Cuesta1, Suzanne S. Gisbertz2 and Donald L. van der Peet1
1Department of Gastro-Intestinal Surgery. VU University Medical Center. Amsterdam, The Netherlands
2Academic Medical Center. Amsterdam, The Netherlands
ABSTRACT
Postoperative complications frequently follow major abdominal surgery and are associated with increased morbidity and mortality. Early diagnosis and treatment of complications is associated with improved patient outcome. In this study we assessed the value of a step-up diagnosis plan by C-reactive protein and CT-scan (computed tomography-scan) imaging for detection of postoperative complications following major abdominal surgery.
An observational cohort study was conducted of 399 consecutive patients undergoing major abdominal surgery between January 2009 and January 2011. Indication for operation, type of surgery, postoperative morbidity, complications according to the Clavien-Dindo classification and mortality were recorded. Clinical parameters were recorded until 14 days postoperatively or until discharge. Regular C-reactive protein (CPR) measurements in peripheral blood and on indication -enhanced CT-scans were performed.
Eighty-three out of 399 (20.6 %) patients developed a major complication in the postoperative course after a median of seven days (IQR 4-9 days). One hundred and thirty two patients received additional examination consisting of enhanced CT-scan imaging, and treatment by surgical reintervention or intensive care observation. CRP levels were significantly higher in patients with postoperative complications. On the second postoperative day CRP levels were on average 197.4 mg/L in the uncomplicated group, 220.9 mg/L in patients with a minor complication and 280.1 mg/L in patients with major complications (p < 0,001). CT-scan imaging showed a sensitivity of 91.7 % and specificity of 100 % in diagnosis of major complications. Based on clinical deterioration and the increase of CRP, an additional enhanced CT-scan offered clear discrimination between patients with major abdominal complications and uncomplicated patients. Adequate treatment could then be accomplished.
Key words: Major abdominal surgery. Postoperative complication. C-reactive protein (CRP). Computed tomography-scan (CT-scan). Quality control.
Introduction
Over the past decades, the medical care for patients undergoing major abdominal surgery has improved significantly with the use of minimally invasive surgical techniques and the Fast Track peroperative care (1). Nevertheless, postoperative complication rates remain high, with a reported incidence of up to 40 % (2). Severe complications which require invasive treatment, such as anastomotic leakage, are reported in up to 19 % of patients, and are associated with increased morbidity and mortality (2,3). Recent studies show a median time of eight days to clinical diagnosis of a complicated postoperative course (3-6). This is especially interesting in the light of Fast-Track care, where patients are discharged early after surgery.
In surgical practice, C-reactive protein (CRP) is used to monitor the postoperative inflammatory phase (4,7,8). CRP levels are deemed valuable in the assessment of grade of inflammation and allow for assessment of the effect of treatment, especially since the levels of CRP are determined only by their rate of synthesis (9). Several studies have addressed the use of CRP in diagnosis of postoperative complications (4,10-15). Statistical differences are reported between uneventful and complicated cases from as early as the second postoperative day, whilst most complications are diagnosed after a median of seven days (5).
Computed tomography (CT) is currently the most readily available imaging in the work-up of major complications (16-18). Moreover, in the study conducted by Eckmann et al., CT-scan imaging showed a sensitivity of 97 % (19). Another recent study established CT-scan imaging as the preferred modality in diagnosis of anastomotic leakage (20). In the study here presented, we assessed the value of clinical parameters and hypothesize a step up diagnosis plan by CRP and CT-scanning in the diagnosis and treatment of postoperative complications after major abdominal surgery.
Materials and methods
Study design
An observational cohort study was conducted of 399 patients undergoing major abdominal surgery in the VU medical centre, Amsterdam between January 2009 and January 2011, with a follow-up of 30 days after admission.
Major abdominal surgery was defined as all digestive resections with reconstruction via primary anastomosis and/or ostomy. For instance, cholecystectomy is not included since no anastomosis or ostomy is performed. Upper GI resections included oesophageal and gastric resections, HPB resections included pancreaticoduodenectomy, partial hepatectomy with anastomosis and duodenectomy, colorectal resections included all small bowel and colon resections with anastomosis and/or ostomy. Both laparoscopic and open procedures, acute and elective performed and malignant and benign diseases were included.
Recorded clinical parameters included indication for operation, type of surgery, duration of surgery, blood loss, clinical parameters, performed CT-scans, complications according to Clavien-Dindo classification and mortality. All parameters were recorded up until the 14th postoperative day, or until discharge, as available. According to local protocol CRP levels and white blood cells (WBC) were determined at the second or third postoperative day (POD) and on demand thereafter. Clinical deterioration, defined as all deviations in vital signs (heart rate, respiratory rate, blood pressure, saturation and temperature) and abdominal findings upon physical examination, such as abdominal tenderness and ileus, and an increase in CRP around 200 mg/L, measured the 2nd or 3rd postoperative day, implicated additional examinations, generally consisting of an enhanced double contrast CT-scan, to assess complications. CT-scans were performed in a Philips 256 slice Brilliance iCT-scanner®, with intravenous contrast and oral and/or rectal contrast.
Since it is particularly important to distinguish complications that require surgical, endoscopic or radiological interventions, complications were scored according to a modified Clavien-Dindo classification in two groups (21,22). Group I consisted of grade I and grade II complications and are classified as "minor complications"; while group II consisted of grade III, IV and V complications, and are classified as "major complications".
All patients received perioperative prophylactic intravenous antibiotics and thromboprophylaxis according to local protocol. Treatments of the major complications were classified as reoperations, radiological interventions such as percutaneous drainage and intensive care admission.
Statistical analysis
Statistical analysis was conducted in SPSS version 19.0 (SPSS Inc. Chicago, IL, USA). Continuous variables with normal distributions were presented as means and standard deviations. Medians and interquartile ranges were used as central tendency for continuous variables with non-normal distributions. Categorical data were expressed with percentage frequencies. Comparison for CRP levels between uncomplicated, minor and major complicated patients was calculated with ANOVA (analysis of variance) tests. Effects between two groups were further examined with a Student's t-test. A value of p < 0.05 was considered statistically significant. χ2-test and McNemar analysis were used for comparing categorical variables as appropriate. The conduct of enhanced CT-scanning was registered regarding indication for scanning, outcome and whether a scan-outcome was an indication to start an intervention. This study was assessed and approved by the medical ethics committee of the VU Medical Centre.
Results
Among 399 patients, seventy-four (18.5 %) had surgery of the upper gastro-intestinal tract (upper GI), ninety-one (22.8 %) cases had hepato-pancreatico-billiary surgery (HPB) and two hundred-and thirty-four patients (58.6 %) had colorectal surgery.
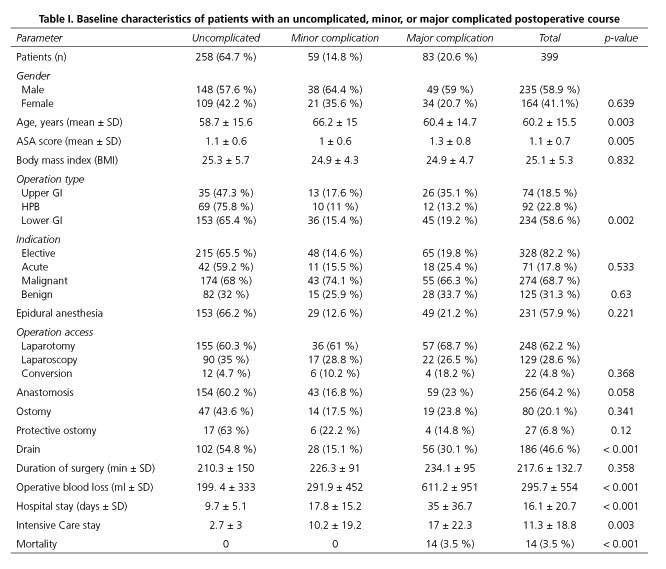
One-hundred-forty-two patients (35.6 %) suffered a complicated postoperative course. Fifty-nine patients (14.8 %) had minor complications, requiring maximally conservative treatment such as medication or wound infections drained at the bedside. Eighty-three patients (20.8 %) experienced a major complication that required invasive treatment or even intensive care admission. Characteristics of patients with uncomplicated, minor or major complicated postoperative course are depicted in table I.
Clinical parameters
Clinical parameters included measurements of heart rate, blood pressure, temperature and abdominal findings such as pain measured with visual analogue scale (VAS) and time to passage of first stool. There were no statistically significant differences between uncomplicated, minor or major complicated patients concerning blood pressure (p > 0.074) or temperature (p > 0.242) or reported VAS-scores (p > 0.05). Heart rate showed statistically significant differences between patients with major complications and those with uncomplicated and minor complications from as early as the first postoperative day (84 beats per minute, bpm) in uncomplicated and minor complications and 90 bpm in patients with a major complication, p = 0.034). Differences in heart rate between the three groups are seen up until postoperative day 5. Figure 1 depicts average measured heart rates and associated p-values. Failure to pass first stool by the third postoperative day was also associated with major complications (p = 0.001). Further analysis of patients who had not passed a first stool by the third postoperative day showed a sensitivity of 69.1 % and specificity of 54.2 %.

Laboratory testing
Blood samples were collected the second or third day postoperatively and thereafter on demand in patients who did not show clinical progression to recovery or showed clinical deterioration. White blood cells (p > 0.087) and creatinine (p > 0.115) did not show statistically significant differences between patients having major, or uncomplicated, or minor complications. Average haemoglobin significantly decreased in patients with major complications from the first postoperative day. All average haemoglobin levels were within the normal range (7.5-10.0 mmol/L). CRP levels showed significant differences between uncomplicated, minor and major complicated patients from as early as the second postoperative day (average CRP levels on POD2 were 196 ± 101 mg/L in uncomplicated cases, 221 ± 122 mg/L in patients with minor complications and 282 ± 95 in patients with major complications), as displayed in figure 2. Average CRP levels on postoperative day two and three were significant between the groups and persist up until sixth postoperative day (p < 0.001). No statistically significant differences were observed in postoperative CRP levels between upper GI, HPB and colorectal surgery (POD2: Average CRP levels in upper GI 201 ± 97 mg/L, in HPB 190 ± 95 mg/L and in colorectal 234 ± 114 mg/L, p = 0.064; POD3: CRP levels in upper GI 186 ± 78 mg/L, in HPB 175 ± 90 mg/L and in colorectal 199 ± 111 mg/L, p = 0,406, all p > 0.05 on further postoperative days). Similar results hold for postoperative CRP levels in laparoscopic and open resections (POD2: average CRP levels in open surgery 226 ± 106 mg/L versus 211 ± 119 mg/L in laparoscopic surgery, p = 0.418; POD3: 198 ± 106 in open surgery versus 181 ± 98 mg/L in laparoscopic surgery, p = 0.320; all p > 0.05 on further postoperative days). CRP levels in patients requiring an acute operation CRP levels were higher on POD1 (144 ± 102 mg/L in acute surgery versus 107 ± 56 in elective surgery, p = 0.034). However, from POD2 onwards no statistically significant differences were observed (POD2 average CRP in acute surgery 248 ± 117 mg/L versus 211 ± 106 mg/L in elective surgery, p = 0.061, all p > 0.05 from POD2 onwards).

CT-scan imaging
Based on clinical deterioration and increased CRP, two-hundred-and-twenty CT-scans were performed in 110 patients. In twenty-seven out of 258 uncomplicated patients a postoperative CT scan was performed (10.6 %) due to clinical deterioration (n = 15) or increasing levels of CRP (n = 9) or both (n = 3). In twelve of these patients CT-scan imaging was considered as normal whereas in the other fifteen patients CT-scans showed abnormalities diagnosed as physiological effects of surgery. In ten patients extra-luminal air was still present, another four patients showed minor fluid collections and in one patient a combination of air and minor fluid. Treatment in these cases was expectative and all patients recovered uneventful. Therefore, no false-positive CT-scans were reported and specificity was calculated at 100 %.
In twenty-two patients out of 59 with minor complications (Clavien-Dindo, grades I and II) a CT-scan was performed (37.3 %) due to clinical deterioration (n = 12), ileus (n = 5), increased levels of CRP (n = 3) or both clinical deterioration and increasing CRP (n = 2). In fifteen patients, CT-scans did not show abnormalities; the complications in these patients were of extra-abdominal origin such as a wound infection in four patients and pneumonia in eight patients. In the other two patients postoperative course was complicated by pneumonia and a wound infection. One patient suffered from both a wound infection and atrial fibrillation. Seven patients did have abnormalities upon CT-scan imaging. Four CT-scans showed signs of intestinal paralysis, treated conservatively; the other two showed bilateral pneumonia in lower lobes, consequently treated with antibiotics and in the last CT-scan a subcutaneous wound infection was seen, which was treated with drainage at the bedside.
Thirty-seven out of 59 patients with a minor complication (Clavien-Dindo grades 1 and 2) did not receive CT-scan imaging. Seventeen of these patients had wound infections consequently drained and the other eight patients had a urinary infection. In another 12 patients pneumonia was diagnosed and other two had both pneumonia and palpitations due to atrial fibrillation.
Sixty-one out of 83 patients with a major complication underwent CT-scan imaging (73 %) due to clinical deterioration (n = 34), increasing CRP levels (n = 13) or both (n = 11) or due to persistent intestinal paralysis (n = 3). Based on the outcome of the CT-scan, thirty-eight patients underwent a reoperation; another twenty patients were treated by percutaneous drainage and in ten patients CT scan was considered as normal. Findings during reoperation were: Twenty patients had an anastomotic leakage with peritonitis, being other thirteen patients reoperated because of abdominal abscesses with intact anastomosis. Two other patients were operated because of small bowel perforation (one perforation of the jejunum and other in the ileum), another two patients because of internal herniation through the diaphragm after oesophageal resection for cancer and the last patient because of postoperative bleeding from the left epigastric artery. Another twenty patients were treated by percutaneous drainage for abscesses (fifteen patients), controlled anastomotic leak with abscess in four and the last patient because of lesion of the left ureter with urinoma. Three patients were admitted to an Intensive Care Unit due to respiratory insufficiency due to pneumonia.
In ten patients CT-scans did not show any abnormalities. In five patients, the major complications were finally diagnosed as extra-abdominal origin such as severe pneumonia in three patients and pneumonia combined with pneumothorax in other two patients, requiring admission on the intensive care. In the other five patients the CT-scan was false negative, these patients suffered from anastomotic leakage (2), intraabdominal abscess (2) and jejunum perforation in the last patient, which significantly delayed diagnosis with a median of seven days (14 days (range 7-23, p = 0.043) whereas in patients with a true positive CT-scan, median of 7 days (range 0-41). The overall sensitivity of the CT-scan is estimated 91.7 % for major complications with a negative predictive value of 90.7 %.
Twenty-two patients with a major complication were directly reoperated because of different reasons. Nine patients were reoperated because of clinical instability and generalized peritonitis. During reoperation four patients had an anastomotic leak, three patients an intestinal perforation (all jejunum), one patient an abscess with no signs of leakage and the last one had a postoperative bleeding of the superior mesenteric artery with hemodynamic shock. Four patients were operated without CT-scan because of clinically evident diagnosis: Three had dehiscence of abdominal wall and other patient had deep necrosis of the colostomy. Another four patients were admitted to the intensive care unit because of respiratory insufficiency with pneumonia. Five patients died before a CT-scan was performed; three due to respiratory insufficiency due to pneumonia and two patients because of sepsis with multiple organ failure. An overview of these patients is depicted in table II.

Mortality
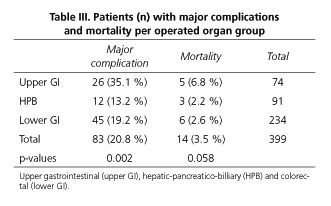
Overall mortality was 3.5 % (fourteen patients). After upper GI surgery five patients (6.8 %) died; three patients due to sepsis following anastomotic leakage; one patient because of respiratory insufficiency with extensive pneumonia and the last patient because myocardial infarction. Three patients (3.3 %) died after HPB surgery; two patients due to postoperative bleeding; and one patient because of respiratory insufficiency with pneumonia. Six patients (2.6 %) died after colorectal surgery; three patients due to respiratory insufficiency with pneumonia; other three because of fulminant sepsis (of these, two patients had an anastomotic leak and one had a colon perforation 15 cm proximal from colostomy). No difference in mortality was observed between the three groups (p = 0.219). An overview of patients with a major complications and mortality rates are depicted in table III.
Discussion
The retrospective observational study here presented supports the role of clinical deterioration or no clinical progression in combination with increased CRP for early detection of major postoperative complications after major abdominal surgery. In an ideal step-up plan clinical deterioration or no clinical progress to recover supported by a postoperative increased CRP at day three or four will be an indication for an enhanced CT-scan imaging to rule out or diagnose a postoperative complication. Clinical parameters, especially heart rate and time to passage of first stool are important clinical markers and showed statistical differences between uncomplicated patients, minor complicated patients and major complicated patients.
In this study 83 patients (20.6 %) had a major complication according to Clavien-Dindo classification requiring reoperation, intervention radiology treatment and/or admission to the intensive care, this being in accordance with current literature (14,15,23). In this study diagnosis of major complications occurred after a median of 7 days (IQR 4-9 days). Early identification and diagnosis of patients with major complications may lead to a decrease in morbidity associated with these complications (23). C-reactive protein has been considered in other studies as an important marker for all postoperative septic complications, for anastomotic leakage, or both with promising results (4,10-12,24,25).
In the postoperative assessment of patients after major abdominal surgery, especially since the implementation of Fast-Track perioperative treatment, the objective must be to achieve a early safe discharge criterion and early diagnosis of major complications, thus aiming for a high negative predictive value and high sensitivity (26). In this series, clinical suspicion and increased CRP, around 200 mg/L was considered as an indication for a CT scan. Average CRP on the third day was 169, 192.7 and 255 mg/L respectively. In the uncomplicated, minor complicated and major complicated group of patients this was an indication for imaging by means of a CT scan in 10.5 %, 37.3 % and 73 % respectively. In the uncomplicated and minor complication group there were no false positive CT scans, but in the major complicated group five patients had a false negative CT scan and this has delayed importantly the time to proper diagnosis with 7 days in comparison with the well diagnosed complication on the CT scan. Consequently enhanced CT-scan showed a sensitivity of 91.7 % for major complications, specificity of 100 % and a false-negative rate of 4.5 %. It has been claimed that early radiological features of major complications may be hard to distinguish from physiological changes following major abdominal surgery (17). In this study, 53.8 % of patients with an uncomplicated postoperative course, CT-scan imaging showed abnormalities, but these were deemed physiological effects of surgical procedure and no treatment was undertaken. These findings are in accordance with literature, for instance pneumoperitoneum is a common finding after major abdominal surgery and may last up to four weeks postoperatively (27). On the other hand, extra-luminal contrast medium can be absent in anastomotic leakage (16,17). Extra watchfulness is warranted in patients with a false-negative scan, but literature and the results here presented indicate that CT-scan is the most adequate aid for diagnosis of postoperative complications (20).
Moreover, not all patients with a major complication needed a CT-scan imaging previous to reoperation. Immediate reoperation can be indicated in for example abdominal wall dehiscence, hemodynamic instability or postoperative bleeding.
Currently, the diagnosis of major complications occurs after a median of seven days (4,10). By implementing a "leakage score", while scoring mainly clinical parameters, Den Dulk et al. managed to decrease the number of days till diagnosis from a median of eight days to a median of six days. Moreover, a delay in relaparotomy was associated with increased morbidity and mortality (28); thereby further supporting the need for a standardized postoperative algorithm (13).
The here presented study has several limitations. For instance data was collected from different surgical procedures, namely upper GI, HPB and lower GI tract. No statistically significant differences in CRP levels were observed between the groups. Similar results hold for laparoscopic and open procedures, again no significant differences in CRP levels were observed. Although patients operated in an acute setting had higher CRP levels on POD1, no differences were observed from POD2 onwards. The observational nature of the study is the main limitation, since CRP measurements were only performed once postoperatively, additional examinations were performed as deemed necessary by the attending physician. This could reflect a lack of data, namely in the absence of clinical symptoms which prompt such a measurement.
Based on the results presented by this study we propose an algorithm for clinical assessment of patients after major abdominal surgery, which includes clinical observation and regular measurements of postoperative CRP, in order to suspect postoperative complications. The absence of daily clinical progress to recovery or clinical deterioration with increased CRP will determine the indication for a CT scan as early as day four. The results of the here presented study showed adequate arguments to correlate the clinical no progress to recovery or deterioration with significant differences in CRP levels between uncomplicated, minor and major complications from as early as the second postoperative day. These two parameters will indicate the necessity to perform an enhanced CT-scan imaging for diagnosis of major complications, while caution is warranted in order to prevent delay in case of false-negative CT-scans. This concept is also important to exclude complications in the fast track concept of early discharge. Hence, in order to ensure early diagnosis of major complications, we propose to perform a randomized control trial to ascertain the proper use of clinical parameters and a to establish cut off CRP at day 3rd or 4th to perform a CT scan in order to diagnose early major complications.
References
1. Vlug MS, Wind J, Hollmann MW, Ubbink DT, Cense HA, Engel AF, et al. Laparoscopy in combination with Fast Track multimodal management is the best perioperative strategy in patients undergoing colonic surgery. (LAFA-study). Ann Surg 2011;254:868-75. [ Links ]
2. Velasco E, Thuler LC, Martins CA, Dias LM, Conalves VM. Risk factors for infectious complications after abdominal surgery for malignant disease. AJIC 1996;24:1-6. [ Links ]
3. Isbister WH. Anastomotic leak in colorectal surgery: A single surgeon's experience. ANZ J Surg 2001;71:516-20. [ Links ]
4. Welsch T, Müller SA, Ulrich A, Kischlat A, Hinz U, Kienle P, et al. C-reactice protein as early predictor for infectious complications in rectal surgery. Int J Colorectal Dis 2007;22:1499-507. [ Links ]
5. Nesbakken A, Nygaard K, Lunde OC, Blucher J, Gjertsen O, Dullerud R. Anastomotic leak following mesorectal excision for rectal cancer: True incidence and diagnostic challenges. Colorectal Disease 2005;7:576-81. [ Links ]
6. Rivers E, Nguyen B, Havstad S, Ressler J, Muzzin A, Knoblich B, et al. Early goal directed therapy in the treatment of severe sepsis and septic shock. NEJM 2001;345:1368-77. [ Links ]
7. Hayashi H, Ochiai T, Shimada H, Gunji Y. Prospective randomized study of open versus laparoscopy-assisted distal gastrectomy with extraperigastric lymph node dissection for early gastric cancer. Surg Endosc 2005;19:1172-6. [ Links ]
8. Kragsbjerg P, Holmberg H, Vikerfors T. Serum concentrations of interleukin-6, tumour necrosis factor alpha and C-reactive protein in patients undergoing major operations. Eur J Surg 1995;161:17-22. [ Links ]
9. Pepys MB, Hirschfield GM. C-reactive protein: A critical update. J Clin Invest 2003;111:1805-12. [ Links ]
10. MacKay GJ, Molloy RG, O'Dwyer PJ. C-reactive protein as a predictor of postoperative infective complications following elective colorectal resection. Colorectal Disease 2011;13:583-7. [ Links ]
11. Ortega-Deballon P, Radais F, Facy O, d'Athis P, Masson D, Charles PE, et al. C-reactive protein is an early predictor of septic complications after elective colorectal surgery. World J Surg 2010;34:808-14. [ Links ]
12. Platt JJ, Ramanathan ML, Crosbie RA, Anderson JH, McKee RF, Horgan PG, et al. C-reactive Protein as a predictor of postoperative infective complications after curative resection in patients with colorectal cancer. Ann Surg Oncol 2012;19:4168-77. [ Links ]
13. Woeste G, Muller C, Bechstein WO, Wullstein C. Increased serum levels of C-reactive protein precede anastomotic leakage in colorectal surgery. World J Surg 2010;34:140-6. [ Links ]
14. Warschkow R, Tarantino I, Ukegjini K, Beutner U, Müller SA, Schmied BM, Steffen T. Diagnostic study and meta-analysis of C-reactive protein as a predictor of postoperative inflammatory complications after gastroesophageal cancer surgery. Langenbecks Arch Surg 2012;397:727-36. [ Links ]
15. Welsch T FK, Frommhold K, Hinz U, Weigand MA, Kleeff J, Friess H, et al. Persisting elevation of C-reactive protein after pancreatic resections can indicate developing inflammatory complications. Surgery 2008;143:20-8. [ Links ]
16. DuBrow RA, David CL, Curley SA. anastomotic leaks after low anterior resection for rectal carcinoma: Evaluation with CT and barium enema. AJR Am J Roentgenol 1995;165:567-71. [ Links ]
17. Power N, Atri M, Ryan S, Haddad R, Smith A. CT assessment of anastomotic bowel leak. Clinical Radiology 2007;62:37-42. [ Links ]
18. Khoury W, Ben-Yehuda A, Ben-Haim M, Klausner JM, Szold O. Abdominal computed tomography for diagnosing postoperative lower gastrointestinal tract leaks. J Gastrointest Surg 2009;13:1454-8. [ Links ]
19. Eckmann C, Kujath P, Schiedeck THK, Shekarriz H, Bruch HP. Anastomotic leakage following low anterior resection: Results of a standardized diagnostic and therapeutic approach. Int J Colorectal Dis 2004;19:128-33. [ Links ]
20. Hyman N, Manchester TL, Osler T, Burns B, Cataldo PA. Anastomotic Leaks after intestinal anastomosis: It's later than you think. Ann Surg 2007;245:254-8. [ Links ]
21. Clavien PA, Barkun J, de Oliveira ML, Vauthey JN, Dindo D, Schulick RD, et al. The Clavien-Dindo classification of surgical complications; five year experience. Ann Surg 2009;250:187-96. [ Links ]
22. Dindo D, Demartines N, Clavien P. Classification of surgical complications; a new proposal with evaluation in a cohort of 6336 patient and results of a survey. Ann Surg 2004;240:205-13. [ Links ]
23. Alves A, Panis YU, Mathieu P, Mantion G, Kwiatkowski F, Slim K. Postoperative mortality in French patients undergoing colorectal surgery. Arch Surg 2005;140:278-83. [ Links ]
24. Warschkow R, Tarantino I, Torzewski M, Näf F, Lange J, Steffen T. Diagnostic accuracy of C-reactive protein and white blood cell counts in the early detection of inflammatory complicationsafter open resection of colorectal cancer: A retrospective study of 1,187 patient. Int J Colorectal Dis 2011;26:1405-13. [ Links ]
25. Kørner H, Nielsen HJ, Søreide JA, Nedrebø BS, Søreide K, Knapp JC. Diagnostic Accuracy of C-reactive protein for intraabdominal infections after colorectal resections. J Gastroinstest Surg 2009;13:1599-606. [ Links ]
26. Warschkow R, Beutner U, Steffen T, Müller SA, Schmied BM, Güller U, et al. Safe and early discharge after colorectal surgery due to C-reactive protein; a diagnostic meta-analysis of 1832 patient. Ann Surg 2012;256:245-50. [ Links ]
27. Cho KC, Baker SK. Extraluminal air: Diagnosis and significance. Radiol Clin North Am 1994;32:829-44. [ Links ]
28. Doeksen A, Tanis PJ, Vrouenraets BC, Lanschot van JJB, Tets van WF. Factors determining delay in relaparotomy for anastomotic leakage after colorectal resection. World J Gastroenterol 2007;13:3721-5. [ Links ]
![]() Correspondence:
Correspondence:
Jennifer Straatman
Department of Gastro-Intestinal Surgery
VU University Medical Center
De Boelelaan 1117
1081 HV Amsterdam, The Netherlands
e-mail: je.straatman@vumc.nl
Received: 23-04-2014
Accepted: 06-07-2014

