










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.107 n.1 Madrid Jan. 2015
Eosinophilic cholecystitis: An infrequent cause of acute cholecystitis
Colecistitis eosinofílica: causa infrecuente de colecistitis aguda
María del-Moral-Martínez1, Andrés Barrientos-Delgado1, Vicente Crespo-Lora2, María Eloísa Cervilla-Sáez-de-Tejada1 and Javier Salmerón-Escobar1
1Digestive Diseases Clinical Management Unit. 2Pathology Clinical Management Unit. Hospital Universitario San Cecilio. Granada, Spain
ABSTRACT
Eosinophilic cholecystitis (EC) is a rare disease that is characterised by eosinophilic infiltration of the gallbladder. Its pathogenesis is unknown, although many hypotheses have been made. Clinical and laboratory manifestations do not differ from those of other causes of cholecystitis. Diagnosis is histological and usually performed after analysis of the surgical specimen. We report the case of a woman aged 24 years, with symptoms of fever, vomiting and pain in the right upper quadrant. When imaging tests revealed acalculous cholecystitis, an urgent cholecystectomy was performed. Histological examination of the surgical specimen revealed eosinophilic cholecystitis. No cause of the symptoms was found.
Key words: Eosinophilic cholecystitis. Acalculous cholecystitis.
RESUMEN
La colecistitis eosinofílica (CE) es una enfermedad rara caracterizada por una infiltración eosinófila de la vesícular biliar. Su etiopatogenia es desconocida, aunque se han postulado múltiples hipótesis. Las manifestaciones clínicas y de laboratorio no difieren de otras causas de colecistitis. El diagnóstico es histológico y suele realizarse tras el análisis de la pieza quirúrgica. Presentamos el caso de una mujer de 24 años, con clínica de fiebre, dolor en hipocondrio derecho y vómitos. Las pruebas de imagen evidenciaban una colecistitis alitiásica, tras lo cual se realizó una colecistectomía urgente. Los hallazgos histológicos de la pieza quirúrgica revelaban una colecistitis eosinofílica. En este caso, no se encontró causa que justificase el cuadro.
Palabras clave: Colecistitis eosinofílica. Colecistitis alitiásica.
Introduction
Eosinophilic cholecystitis is an uncommon condition of the gallbladder. It is characterised by an inflammatory infiltrate constituted mainly of eosinophils. Its aetiology is often unknown, although cases have been associated with hyper-eosinophilic syndrome, parasitosis, infections, drugs and medicinal herbs. Clinically, it is indistinguishable from common cholecystitis, although peripheral eosinophilia is sometimes observed, as is the case in hyper-eosinophilic syndrome and parasitic disease. When the effect is limited to the bladder, the treatment of choice is cholecystectomy, and the prognosis is usually favourable.
Case report
A 24-year-old woman presented to the emergency department complaining of abdominal pain, located in the epigastrium and radiating to the right upper quadrant, together with nausea, vomiting and fever of 39 oC for the past two days. The presence of choluria was also reported. The patient had no personal or family history of interest. She smoked about five cigarettes per day and was a habitual consumer of oral contraceptives. Physical examination revealed good general condition, with cutaneous-mucous jaundice and tenderness in the right upper quadrant, and a positive Murphy sign. Other results of the examination were normal. Laboratory analysis revealed the following alterations: Total bilirubin 3.76 mg/dL (range 0-1.2 mg/dL); direct bilirubin 3.5 mg/dL (range 0-0.5 mg/dL); indirect bilirubin 0.26 mg/dL (range 0-0.75 mg/dL); alanine aminotransferase 174 U/l (range 0-35 U/l); amylase 49 U/L (range 28-100 U/L); C-reactive protein 149.12 mg/L (range 0-5 mg/L); leukocytes 15,500 µl (range 4.8-10.8 µl); neutrophils 86.3 % (range 40-74 %); lymphocytes 4.2 % (range 19-48 %); monocytes 6.9 % (range 1-9 %); eosinophils 2.2 % (range 0-7 %); prothrombin activity 60.8 % (range 70-120 %), INR 1.34 (range 0.85-1.2); APTT 28.2 sec (range 23.5-33.2 sec). Abdominal ultrasound findings: Thin-walled acalculous gallbladder; non-dilated bile duct; no evidence of pancreatic abnormalities. In view of the clinical and laboratory findings, the patient was admitted to monitor the evolution of the condition and for further study.
During admission, abdominal and cholangio MRI were performed to assess the bile duct, obtaining the following results: no dilatation; no evidence of bile duct filling defects; space-occupying lesion of 9 mm in segment 8 with uptake and density suggesting hemangioma; no evidence of alterations in pancreas or liver. Further analyses were performed, which revealed increased total bilirubin, decreased direct bilirubin, increased leukocytosis, increased C-reactive protein, and normal levels of amylase, transaminases and cholestatic enzymes. The patient had malaise, with increased pain despite analgesia, and painful abdominal tenderness, with a tightening in the epigastric right upper quadrant. In view of this situation, an urgent abdominal CT scan with IV contrast was performed (Fig. 1), which showed perivesicular oedema without calculi or biliary dilatation, with a small amount of free fluid in the Douglas pouch. There were no images suggestive of perforation or pancreatitis.

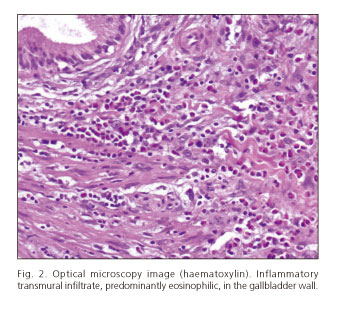
The patient's clinical condition was worsening and presence of cholecystitis was suspected, and so an urgent cholecystectomy was performed, which revealed a thickened gallbladder wall with oedema on the rear surface. The pathology examination revealed the presence of a transmural infiltration, and of a more intense infiltration in the muscular layer, by eosinophilic polynuclear leukocytes (Fig. 2).
After surgery, the patient was asymptomatic and was discharged a few days later.
Discussion
Eosinophilic cholecystitis (EC) is a rare and poorly understood disease of the gallbladder, which was first described in 1949. It can be considered an inflammatory condition of the gallbladder, in which the inflammatory infiltrate consists primarily of eosinophils (1).
The aetiology of EC is unknown. In patients with eosinophilic infiltrate affecting other organs and tissues, it has been suggested that these lesions could be due to a local allergic reaction to substances released at sites of inflammation within the target organ or tissue. It has also been hypothesised that EC may be caused by hypersensitivity to bile acids (2,3).
Cases have also been reported secondary to infections, parasitosis, allergies, hyper-eosinophilic syndrome, eosinophilia-myalgia syndrome, eosinophilic gastroenteritis, drugs and herbal medicines (4,5). In the absence of evident causes, we consider the present case to be an idiopathic EC (6).
EC is three times more common in patients with acalculous cholecystitis than in patients with cholelithiasis (6).
EC does not present any clinical or laboratory manifestation to distinguish it from common cholecystitis, and so it is difficult to detect prior to cholecystectomy and histological examination of the surgical specimen. Peripheral eosinophilia may or may not be present; when it is, it has been associated with hyper-eosinophilic syndrome, eosinophilic gastroenteritis and parasitosis. In addition, symptoms secondary to the eosinophilic infiltration of other organs have been described (8).
Diagnosis is histological; EC is said to be present when the cellular infiltrate in the gallbladder wall is composed of more than 90 % eosinophils, and the cholecystitis is chronic with an eosinophilic (lympho-eosinophilic) component if the infiltrating inflammatory leukocyte population contains 50-75 % eosinophils (9). In imaging tests, ultrasound results may be normal or show signs suggestive of cholecystitis (gallbladder distension, wall thickening, perivesicular liquid or sonographic Murphy sign). A CT scan may reveal similar features, with perivesicular oedema or decreased attenuation in the adjacent liver, indicative of perihepatitis (10).
EC prognosis is favourable. When the disease is confined to the bladder, the treatment of choice is cholecystectomy, preferably performed laparoscopically. Treatment with corticosteroids can be effective when the bile ducts are affected, or when the condition is associated with eosinophilic gastroenteritis.
It is generally accepted that EC should not be considered a separate entity, because the clinical and laboratory manifestations are indistinguishable from those of common cholecystitis, and therefore it is considered more a histological finding than a pathology in itself. The importance of EC lies in the fact that it can be associated with other diseases, and therefore, when it is observed, possible associated syndromes should be investigated.
References
1. Albot G, Poilleux H, Oliver C. Les cholécystites a éosinophils. Presse Med 1949;57:558-9. [ Links ]
2. Pardo-Mindan FJ, Joly MA, Santamaria M, Munoz Navas M. Eosinophil inflammatory reaction in isolated organs. Allergol Immunopathol (Madr.) 1980;8:23-30. [ Links ]
3. Alfaro J, Fernández L, Hörndler C, Ruiz JM, Sanz JM, López M, et al. Eosinophilic cholecystitis associated with rupture of hepatic hydatid cyst of the bile ducts. Rev Esp Enferm Dig 1995;87:889-90. [ Links ]
4. Adusumilli PS, Lee B, Parekh K, Farrelly PA. Acalculous eosinophilic cholecystitis from herbal medicine: a review of adverse effects of herbal medicine in surgical patients. Surgery 2002;131:352-6. [ Links ]
5. Hepburn A, Coady A, Livingstone J, Pandit N. Eosinophilic cholecystitis as a possible late manifestation of the eosinophilia-myalgia syndrome. Clin Rheumatol 2000;19:470-2. [ Links ]
6. Sánchez-Pobre P, López-Ríos Moreno F, Colina F, Yela C, Manzano M, et al. Eosinophilic cholecystitis: An infrequent cause of cholecystectomy. Gastroenterol Hepatol 1997;20:21-3. [ Links ]
7. Singh DK, Shankar R, Gondal R, Malhotra V, Mishra P. Idiopathic eosinophilic cholecystitis with cholelithiasis: A case report and review of literature. The Internet Journal of Surgery. 2008;16. [ Links ]
8. Shakov R, Simoni G, Villacin A, Baddoura W. Eosinophilic cholecystitis, with a review of the literature. Ann Clin Lab Sc 2007;37:182-5. [ Links ]
9. Punia RP, Arya S, Jain P, Bal A, Mohan H. Eosinophilic and lympho-eosinophilic cholecystitis. Indian J Gastroenterol 2003;22:153-4. [ Links ]
10. Patel NB, Oto A, Thomas S. Multidetector CT of emergent biliary pathologic conditions. Radiographics 2013;33:1867-88. [ Links ]
![]() Correspondence:
Correspondence:
María del-Moral-Martínez.
Digestive Diseases Clinical Management Unit.
Hospital Universitario San Cecilio.
Avda. Doctor Oloriz, 16.
18012 Granada, Spain
e-mail:
mdelmoral87@gmail.com
Received: 05-03-2014
Accepted: 23-06-2014

