










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.107 no.2 Madrid feb. 2015
Oropharyngeal dysphagia, an underestimated disorder in pediatrics
Disfagia orofaríngea, un trastorno infravalorado en pediatría
Esther Vaquero-Sosa1, Laura Francisco-González1, Andrés Bodas-Pinedo1, Cristina Urbasos-Garzón2 and Antonio Ruiz-de-León-San-Juan3
1Gastroenterology and Nutrition Unit. Department of Pediatrics.
2Department of Otorrinolaringology
3Department of Digestive Diseases.
Hospital Clínico San Carlos. Madrid, Spain
ABSTRACT
Oropharyngeal dysphagia is a rather frequent clinical entity in patients with neurological problems that can lead to serious complications such as aspiration pneumonia and other disorders like dehydration or malnutrition due to feeding difficulties. It should be suspected in children with splitting of food intake or prolonged feeding, coughing or choking during feeding, continuous drooling or repeated respiratory symptoms. For the diagnosis, apart from the examination of swallowing, additional tests can be run like the water-swallowing test, the viscosity-volume test (which determines what kind of texture and how much volume the patient is able to tolerate), a fiberoptic endoscopy of swallowing or a videofluoroscopic swallow study, which is the gold standard for the study of swallowing disorders.
It requires a multidisciplinary approach to guarantee an adequate intake of fluids and nutrients with minimal risk of aspiration. If these two conditions cannot be met, a gastrostomy feeding may be necessary.
Key words: Oropharyngeal dysphagia. Pediatrics. Management. Aspiration. Pneumonia. Videofluoroscopy.
RESUMEN
La disfagia orofaríngea es una entidad clínica bastante frecuente en pacientes con problemas neurológicos, que puede conllevar complicaciones graves como las neumonías aspirativas y otras alteraciones como deshidratación o desnutrición por dificultades para la alimentación. Debe sospecharse en niños con fraccionamiento de la toma o ingestas prolongadas, tos o atragantamientos asociados a la alimentación, babeo continuo o sintomatología respiratoria de repetición. Para su diagnóstico, además de la exploración de la deglución, pueden hacerse pruebas complementarias como la prueba de deglución del agua, la de viscosidad-volumen (determina qué tipo de textura y cuánto volumen puede tolerar el paciente), la fibroendoscopia de la deglución y la videofluoroscopia (el gold estándar para el estudio de los trastornos de la deglución).
Requiere un abordaje multidisciplinar para asegurar un adecuado aporte oral de líquido y nutrientes, con mínimo riesgo de aspiración. Si estas dos condiciones no son posibles puede ser necesaria la alimentación por gastrostomía.
Palabras clave: Disfagia orofaríngea. Pediatría. Manejo. Neumonía aspirativa. Videofluoroscopia.
Introduction
Swallowing occurs along three phases -oral, pharyngeal, and esophageal. Oropharyngeal dysphagia involves the initial two phases and is rather common in patients with neurological impairment (1). Despite this, the condition is usually underestimated in the pediatric setting, and may result in serious complications such as dehydration, malnutrition, and respiratory disorders. An appropriate patient assessment should allow confirmation of this diagnosis and the development of an adequate treatment plan on an individual basis (2,3).
Case report
We report the case of a 7-year 10-month-old child with a history of mitochondrial cytopathy (respiratory chain complex I-III-IV deficiency) on vitamins B1 and B6, carnitine, coenzyme Q, clobazam, and phenobarbital. The patient was referred for assessment to the Pediatric Gastroenterology and Nutrition clinic because of choking episodes while eating and several admissions for pneumonia. During history taking the patient's parents reported they were feeding their son with purées, but then he had cough bouts and raspiness on swallowing. Upon physical examination the patient was in good general condition with no signs of dehydration or malnutrition, and exhibited age- and gender-appropriate anthropometric percentiles. Abnormal findings included generalized hypotonia, phonoarticulatory and swallowing apraxia, and oral hypotonia with drooling. The exam yielded no other findings.
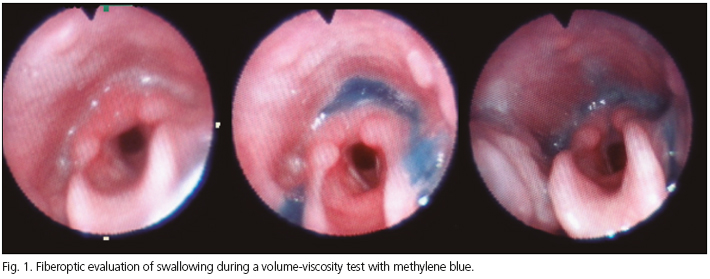
From all the above oropharyngeal dysphagia was suspected and, with no video-fluoroscopy available at that moment in our site, a fiberoptic endoscopic evaluation of swallowing (FEES) procedure was performed during deglutition testing with various volumes and textures (Fig. 1). At rest secretions were seen in the vallecula, pharynx, and pyriform sinuses; following the administration of different methylene blue-stained consistencies and volumes it was concluded that 5 cc of a nectar texture resulted in a slow, highly fractionated swallowing reflex with no cough reflex; food initially remained in the vallecula, pharynx, and pyriform sinuses (subsequently passing into the esophagus under the effect of gravity). With 5 cc of pudding (thicker texture) there was penetration without cough reflex; fractionated swallowing with pooling in the vallecula, pharynx, and pyriform sinuses; delayed progression into the esophagus, and deficient upper esophageal sphincter opening.
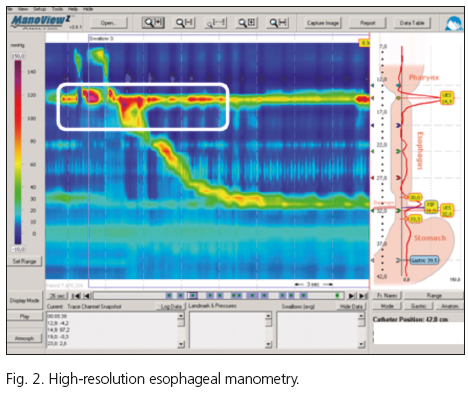
Given his underlying neurological disorder, the patient also underwent high-resolution manometry (Fig. 2) to assess esophageal motility. This test resulted in findings suggestive of hypertensive upper esophageal sphincter with poor pharyngeal pumping and normal peristaltic waves alternating with very low amplitude contractions. Resting pressure in the esophageal body was normal whereas that in the lower esophageal sphincter was on the lower limit of normal.
The patient was diagnosed with oropharyngeal dysphagia of neurogenic etiology and a multidisciplinary approach was established. A liquid thickener was prescribed together with a hypercaloric diet with nectar texture in small volumes, which had been seen to provide the lowest aspiration risk during swallowing tests. General measures were recommended, including avoidance of dual textures and appropriate posturing at meals (upright trunk, symmetric shoulders, slightly flexed head), and the patient was also referred to logopedia for swallowing rehabilitation exercises.
The outcome was favorable in subsequent years; he has mild choking episodes but no admissions for aspiration pneumonia and no other complications such as dehydration or malnutrition, hence no gastrostomy has been considered.
Discussion
The impairment of the oral and pharyngeal stages of deglutition (oropharyngeal dysphagia) may entail serious complications, including aspiration pneumonia and disorders such as dehydration and malnutrition because of difficulties with food. Identifying children at risk for dysphagia, performing the appropriate tests, and setting up a multidisciplinary management plan is of great importance (4).
Oropharyngeal dysphagia should be suspected in children with splitting of prolonged ingestions and food-associated cough or choking, ongoing drooling, or repeated respiratory manifestations (5). It is a lot more common in preterm newborns and children with underlying neurological disorders (6), with some series showing a prevalence of 85 % in patients with cerebral palsy (7).
When clinically suspected the strength and resistance of the tongue and maxillaries, the palatoglossal seal, and the palatal reflex. Examining deglutition is also important; a water test may reveal signs suggestive of oropharyngeal dysphagia such as drooling, cough, dysphonia, or fractionated swallowing (8). The volume-viscosity swallow test includes the progressive administration of various textures (nectar, honey, pudding) in growing volumes (5, 10, 20 ml) according to swallowing efficacy and safety (9). This testing may be performed with pulse oximetry to assess potential desaturations (over 5 %) as indirect evidence of aspiration.
Fiberoptic endoscopic assessment of swallowing (FEES) is useful to visualize deglutition dynamics, bolus penetration, pharyngeal residue, and the efficacy of airway protection mechanisms. Video-fluoroscopy is considered the gold standard, but is available only in few centers and requires brevity to avoid excessive radiation exposure to the thyroid gland (10). It consists of a dynamic study of deglutition (which includes the oral phase as opposed to FEES) by administering a bolus marked with a water-soluble contrast medium (11). In addition to confirming the diagnosis of dysphagia, the test can also detect silent aspiration, a common occurrence in neurologic patients that is easily overlooked given that no symptoms or desaturations result (12,13). In a recent study, high-resolution manometry combined with impedance was also considered a useful technique for the assessment of aspiration risk in patients with oropharyngeal dysphagia (14).
In the pediatric setting, this disorder requires a multidisciplinary management to ensure the child is receiving an adequate provision of oral liquids and nutrients while keeping aspiration risk at a minimum. Should the patient be unable to orally ingest enough calories for adequate growth and development in a safe, aspiration-free manner, gastrostomy may be the treatment of choice (4,15). The volume and texture to be administered are established according to the findings obtained during the swallow test (fiberoptic endoscopic assessment or video-fluoroscopy) in order to minimize the risk for aspiration into the airway tree (3,16). In this respect posturing is also important at meals, as are exercises aimed at strengthening swallowing muscles (15).
To conclude, early dysphagia identification should be based on the data obtained from the patient's medical history and the findings of swallow testing with either the water test or the volume-viscosity test, with subsequent confirmation by diagnostic methods such as fiberoptic endoscopy or video-fluoroscopy. Following these tests food ingestion should be adjusted to provide water and nutritional requirements while avoiding aspiration risks into the airway. Gastrostomy must be considered when these goals are unmet.
References
1. Calis EA, Veugelers R, Sheppard JJ, Tibboel D, Evenhuis HM, Penning C. Dysphagia in children with severe generalized cerebral palsy and intellectual disability. Dev Med Chil Neurol 2008;50:625-30. [ Links ]
2. Dusick A. Investigation and management of dysphagia. Sem Ped Neurol 2003;10:255-64. [ Links ]
3. Laborda González L, Gómez Enterría P. Tratamiento nutricional de la disfagia orofaríngea. Endocrinol Nutr 2006;53:309-14. [ Links ]
4. Arvedson JC. Assessment of pediatric dysphagia and feeding disorders: Clinical and instrumental approaches. Dev Disabil Res Rev 2008;14:118-27. [ Links ]
5. Prasse JE, Kikano GE. An overview of pediatric dysphagia. Clin Pediatr (Phila) 2009;48:247-51. [ Links ]
6. Kakodkar K, Schroeder JW Jr. Pediatric dysphagia. Pediatr Clin North Am 2013;60:969-77. [ Links ]
7. Benfer KA, Weir KA, Bell KL, Ware RS, Davies PS, Boyd RN. Oropharyngeal dysphagia and gross motor skills in children with cerebral palsy. Pediatrics 2013;131:1553-62. [ Links ]
8. Suiter DM, Leder SB, Karas DE. The 3-ounce (90-cc) water swallow challenge: A screening test for children with suspected oropharyngeal dysphagia. Otolaryngol Head Neck Surg 2009;140:187-90. [ Links ]
9. Clavé P, Arreola V, Romea M, Medina L, Palomera E, Serra-Prat M. Accuracy of the volumen-viscosity swallow test for clinical screening of oropharyngeal dysphagia and aspiration. Clin Nutr 2008;27:806-15. [ Links ]
10. Clarke R. 21st century challenges in radiation protection and shielding: Draft 2005 recommendations of ICRP. Radiat Prot Dosimetry 2005;115:10-5. [ Links ]
11. Rugiu MG. Role of videofluoroscopy in evaluation of neurologic dysphagia. Acta Otorhinolaryngol Ital 2007;27:306-16. [ Links ]
12. Silva AB, Piovesana AM, Barcelos IH, Capellini SA. Clinical and videofluoroscopic evaluation of swallowing in patients with spastic tetraparetic cerebral palsy and athetosic cerebral palsy. Rev Neurol 2006;42:462-5. [ Links ]
13. Kim JS, Han ZA, Song DH, Oh HM, Chung ME. Characteristic of dysphagia in children with cerebral palsy, related to gross motor function. Am J Phys Med Rehabil 2013;92:912-9. [ Links ]
14. Rommel N, Selleslagh M, Hoffman I, Smet MH, Davidson G, Tack J, et al. Objective assessment of swallow function in children with suspected aspiration using pharyngeal automated impedance manometry. J Pediatr Gastroenterol Nutr 2014;58:789-94. [ Links ]
15. Newman LA. Optimal care patterns in pediatric patients with dysphagia. Semin Speech Lang 2000;21:281-91. [ Links ]
16. Kirby M, Noel RJ. Nutrition and gastrointestinal tract assessment and management of children with dysphagia. Semin Speech Lang 2007;28:180-9. [ Links ]
![]() Correspondence:
Correspondence:
Esther Vaquero Sosa
Gastroenterology and Nutrition Unit
Department of Pediatrics
Hospital Clínico San Carlos
C/ Doctor Martín Lagos, s/n.
28040 Madrid, Spain
e-mail: estvaqsos@yahoo.es
Received: 04-04-2014
Accepted: 06-07-2014

