










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.107 n.11 Madrid Nov. 2015
Small bowel obstruction due to laparoscopic barbed sutures: An unknown complication?
Juan José Segura-Sampedro1,2, Hutan Ashrafian3,5, Antonio Navarro-Sánchez4,5, John T. Jenkins4, Salvador Morales-Conde2 and Alberto Martínez-Isla4,5
1 Department of Surgery. Hospital Universitario Son Espases. Palma, Islas Baleares. Spain.
2 Department of Surgery. Hospital Universitario Virgen del Rocío. Sevilla, Spain.
3 Department of Surgery and Cancer. Imperial College London. St Mary's Hospital. London, UK.
4 Department of Surgery. St. Mark's Hospital. Harrow, UK.
5 Northwick Park and St. Mark's Hospital. North West London Hospitals NHS Trust. London, UK
ABSTRACT
Background: In recent years there has been an increasing uptake in the use of barbed sutures, particularly in minimally invasive and laparoscopic procedures where they may reduce operating time and improve surgical efficiency. However, little is known about the adverse events associated with these new materials and concerns have arisen regarding their safety in certain procedures.
Methods: We performed a search of electronic databases (PubMed, EMBASE, and Cochrane Database). We reveal up to 15 cases of small bowel obstruction (SBO) complicating laparoscopic pelvic surgery that have been reported to date adding two cases of SBO in our own practice following the use of barbed sutures in laparoscopic operations, both requiring surgical re-intervention in the early post-operative period.
Results: Fifteen similar cases of small bowel obstruction were identified, all of which occurred in patients undergoing surgery below the transverse colon. Surgical re-intervention was required in all cases although 60% of these were performed laparoscopically.
Conclusions: These cases highlight that although barbed sutures provide an attractive means to allow easier and faster laparoscopic suturing, they should be used carefully in inframesocolic surgery and the suture end cut and buried to avoid inadvertent attachment to the small bowel or its mesentery. Barbed suture entanglement should be considered as an uncommon yet potentially serious differential cause for SBO presenting in the early period after laparoscopic surgery where a barbed suture has been used.
Key words: Barbed suture. Small bowel obstruction. Surgery. Complication.
Background
Barbed sutures were first described as early as 1951 (1), and have evolved to become part of every day operative practice, particularly in laparoscopic surgery. The anchoring property of these materials obviates the need for a conventional surgical knot and provides tissue approximation and traction without requiring an assistant, thus improving surgical efficiency. This is of particular benefit in minimally invasive procedures where constraints of space and manoeuvrability may present particular technical challenges. Currently, two types of barbed suture are most commonly employed in gastrointestinal surgery, namely V-loc® (2) and Quill® (3). However, despite their rapid uptake, little is known about the potential complications associated with these materials and concerns have begun to arise regarding their safety in som e procedures.
Postoperative small bowel obstruction is common and has often been linked to the presence of foreign materials, particularly surgical mesh (4). Here we report two cases of small bowel obstruction (SBO) subsequently requiring surgical re-intervention that may be directly related to the use of barbed sutures. In both cases these complications arose from adherence of the suture's distal end to small bowel and mesentery. Review of the current literature highlights this is not an isolated phenomenon, identifying 15 reports of similar cases describing isolated SBO secondary to the intra-peritoneal use of barbed sutures. The aims of this study are therefore to draw attention to this relatively under recognised complication and to outline the mainstay of management in these patients.
Case report
Case report 1
A 58 year-old Caucasian lady presented to our hospital with a rectal prolapse requiring surgical correction. Routine laparoscopic posterior fixation rectopexy was performed with full circumferential rectal mobilization to the pelvic floor without intraoperative complications. The retracted mesorectum was then fixed to the presacral fascia using five midline Ethibond 3/0 suture (add details). The pelvic peritoneum was then closed after using V-loc sutures with the peritoneal closure finishing above the pelvic brim. The V-loc was cut short (< 0.5 cm) at this point. Despite making a good initial recovery with discharge on postoperative day two, on day ten the patient developed diffuse abdominal pain and distention requiring readmission, with evidence of small bowel dilatation on plain abdominal X-ray. Given the worsening of her clinical state and blood biochemistry, she was taken back to theatre for exploratory laparotomy. Intra-operatively, she had obstructed and volved the distal small bowel with subsequent strangulation and infarction. The cut end of the V-loc® suture above the pelvic brim was found to be tightly adherent to the small bowel and wrapped around the serosa causing obstruction and strangulation. 90 cm of strangulated small bowel was resected and a double-barrelled jejuno-ileostomy was fashioned. Post-operatively she made a slow recovery and was eventually discharged on after two months in hospital without further complications. Her jejuno-ileostomy was reversed four months after discharge via a peristomal approach.
Case report 2
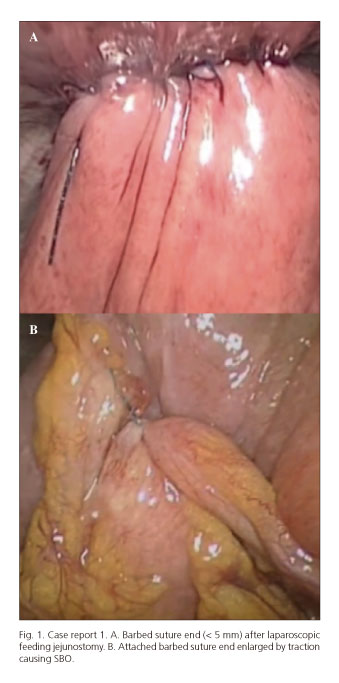
76 year-old lady with maxillofacial cancer requiring feeding jejunostomy. Laparoscopic jejunostomy was performed with fixation of the small bowel to the anterior abdominal wall using a V-loc® barbed suture (Fig. 1). On post-operative day two, the patient developed diffuse abdominal pain and distension with associated vomiting and intolerance of her feed. She failed to improve with conservative management, and oral contrast-enhanced abdominal computerised tomography (CT) performed on day 5 demonstrated small bowel obstruction with suspected volvulus. She was returned to theatre for laparoscopic exploration. SBO was noted secondary to the cut end of V-loc® suture, which had become integrated into the small bowel serosa creating a volvulus with associated ischaemia (Fig. 1). Release of the adherent suture resulted in good re-perfusion and no resection was required. The serosal injury was oversewn. Post-operatively the patient had an uneventful recovery and was discharged on day two without further complication.
Discussion
These two cases highlight a potentially severe complication occurring secondary to the use of barbed sutures in the intra-peritoneal cavity. Although uncommon, a literature search of PubMed, EMBASE, Google Scholar and the Cochrane Central Register of Controlled Trials identified 15 similar cases of small bowel obstruction, all of which occurred in patients undergoing surgery below the transverse colon (Table I). Surgical re-intervention was required in all cases although 60% of these were performed laparoscopically.
The mechanism of SBO documented in these cases is comparable to that described here. Where the cut end of the barbed suture is left long, it may become firmly attached to underlying small bowel or mesentery producing kinking and a transition point of obstruction. Torsion of the small bowel around this point of fixation may result in volvulus and where mesenteric blood flow is impeded, ischemia may occur. In one unusual case, the authors also noted entanglement between the cut ends of two V-loc sutures, producing a transition point and subsequent SBO (9). Although all cases resulted in surgical intervention, the mainstay of treatment is simple division of the embedded barbed suture and liberation of the entrapped bowel. Only in three cases small bowel resection was required. To prevent recurrence, the barbed suture may be additionally trimmed and buried either using absorbable sutures, or surgical clips (7).
The cases presented in this review highlight the potential for SBO to occur as a complication of the use of barbed sutures in laparoscopic surgery. Although these materials may improve surgical efficiency by facilitating tissue approximation particularly during laparoscopic procedures, the ability for the barbs to become non-specifically attached to surrounding tissue is of particular concern when in anatomical proximity to the small bowel and its mesentery. Where barbed sutures are used in the inframesocolic region, we therefore recommend precautions be taken so as to reduce the risk of SBO. In the case of V-loc sutures, we advocate that the ends are either buried, oversewn or cut flush with the tissue in which it is used (5). Notably, other authors have proposed alternative approaches to cover the suture end with either a cellulose sheath such as Surgicel (6), or a laparoscopic clip such as the LAPRA-TY® device (7).
Conclusion
As with any novel drug treatment, it is paramount that surgeons remain vigilant of and report the occurrence of previously unrecognised complications when new surgical devices or materials are introduced. In the case of SBO complicating the early period after laparoscopic inframesocolic surgery, it is important to consider barbed suture entanglement as a potential aetiology for this condition and maintain a high index of suspicion when reviewing post-operative imaging in these cases. We suggest that precautionary measures are taken to cover the ends of barbed sutures during inframesocolic surgery in order to optimise the benefits of this surgical technology.
References
1. Mansberger AR, Jennings ER, Smith EP, et al. A new type pull-out wire for tendon surgery; a preliminary report. Bulletin of the School of Medicine 1951;36:119-21. [ Links ]
2. Demyttenaere SV, Nau P, Henn M, et al. Barbed suture for gastrointestinal closure: a randomized control trial. Surg Innov 2009;16:237-42. DOI: 10.1177/1553350609342988. [ Links ]
3. Moran ME, Marsh C, Perrotti M. Bidirectional-barbed sutured knotless running anastomosis v classic Van Velthoven suturing in a model system. J Endourol 2007;21:1175-8. DOI: 10.1089/end.2007.9913. [ Links ]
4. Luijendijk RW, de Lange DC, Wauters CC, et al. Foreign material in postoperative adhesions. Ann Surg 1996;223:242-8. DOI: 10.1097/00000658-199603000-00003. [ Links ]
5. Vasudevan SP, Dworkin MJ. Small bowel obstruction following laparoscopic ventral mesh rectopexy. Colorectal Dis 2013;15:1543-4. DOI: 10.1111/codi.12402. [ Links ]
6. Bassi A, Tulandi T. Evaluation of total laparoscopic hysterectomy with and without the use of barbed suture. J Obstet Gynaecol Can 2013;35:718-22. [ Links ]
7. Donnellan NM, Mansuria SM. Small bowel obstruction resulting from laparoscopic vaginal cuff closure with a barbed suture. J Minim Invasive Gynecol 2011;18:528-30. DOI: 10.1016/j.jmig.2011.03.011. [ Links ]
8. Kindinger LM, Setchell TE, Miskry TS. Bowel obstruction due to entanglement with unidirectional barbed suture following laparoscopic myomectomy. Gynecol Surg 2012;9:357-8. DOI: 10.1007/s10397-012-0733-9. [ Links ]
9. Ovesen RI, Friis-Andersen H. Ileus caused by V-loc sutures. Ugeskr Læger 2014;176. [ Links ]
10. Rombaut S, Baulies S, Cusidó M, et al. Quill barbed suture-related complication. Gynecol Surg 2012;9:359-1. DOI: 10.1007/s10397-012-0749-1. [ Links ]
11. Thubert T, Pourcher G, Deffieux X. Small bowel volvulus following peritoneal closure using absorbable knotless device during laparoscopic sacral colpopexy. Int Urogynecol J 2011;22:761-3. DOI: 10.1007/s00192-010-1348-1. [ Links ]
12. Buchs NC, Ostermann S, Hauser J, et al. Intestinal obstruction following use of laparoscopic barbed suture: a new complication with new material? Minim Invasive Ther Allied Technol 2012;21:369-71. DOI: 10.3109/13645706.2011.638643. [ Links ]
13. Burchett MA, Mattar SG, McKenna DT. Iatrogenic intestinal and mesenteric injuries with small bowel volvulus following use of barbed suture during laparoscopic myomectomy. J Laparoendosc Adv Surg Tech A 2013;23:632-4. DOI: 10.1089/lap.2013.0065. [ Links ]
14. Salminen HJ, Tan WS, Jayne DG. Three cases of small bowel obstruction after laparoscopic ventral rectopexy using the V-Loc® suture. Tech Coloproctol 2014:18:601-2. DOI: 10.1007/s10151-013-1074-z. [ Links ]
15. Quibel S, Roman H, Marpeau L. Volvulus following barbed suture. Gynecol Obstet Fertil 2012;40:382-3. DOI: 10.1016/j.gyobfe.2012.04.003. [ Links ]
![]() Correspondence:
Correspondence:
Juan José Segura-Sampedro.
Department of Surgery.
Hospital Universitario Son Espases.
Carr. de Valldemossa, 79.
07120 Palma, Islas Baleares. Spain
e-mail: segusamjj@gmail.com
Received: 23-05-2015
Accepted: 22-06-2015

