










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.108 n.1 Madrid Jan. 2016
ORIGINAL PAPERS
Efficacy of a high-resolution consultation system in gastroenterology at an Andalusian hospital center
Eficacia de un sistema de consultas de alta resolución en gastroenterología en un centro hospitalario andaluz
José Luis Zambrana-García1, María Isabel Montoro-Caba2, Maite Chicano-Gallardo3, Ana Monrobel-Lancho3, Daniel Jesús Pérez-de-Luque3, Jose Antonio Peña-Ojeda3 and José Manuel Recio-Ramírez4
1Assistance Coordination Unit. Hospital de Montilla. Montilla, Córdoba. Spain.
2Family and Community Medicine Teaching Unit. Córdoba, Spain.
3Division of Digestive Diseases and
4Critical and Urgent Processes Unit. Hospital de Montilla. Montilla, Córdoba. Spain
ABSTRACT
Background: By high resolution consultation (HRC) we mean an ambulatory process of assistance fulfilled in a single day, by which treatment and diagnosis are established and recorded.
Objective: To assess to which extent patients with digestive conditions may benefit from a single consultation system.
Material: A descriptive study of 179 first visit events, randomly selected as high-resolution consultations in gastroenterology. We discuss the percentage of patients who benefited from HRC and the complementary tests performed.
Results: Most common conditions included dyspepsia (16%), a family history of colon cancer (16%) and gastroesophageal reflux disease (GERD) (16%). Seventy-nine (44%) of all first visits became HRCs and 80 (45%) required a diagnostic test (100% abdominal ultrasound) that was reviewed on the same day. Performing a test on the same day significantly increased the percentage of HRCs (57% vs. 34%, p < 0.002). GERD, dyspepsia, cholelithiasis and chronic liver disease were the subjects most commonly leading to HRC.
Conclusions: Gastroenterology consultations may largely benefit from an HRC system with only organizational changes and no additional costs.
Key words: High-resolution consultation. Single consultation. Gastroenterology consultation.
RESUMEN
Antecedentes: la consulta alta resolución o única es aquel proceso asistencial ambulatorio en el que queda establecido un diagnóstico junto con su correspondiente tratamiento y reflejados ambos en un informe clínico, siendo realizadas estas actividades en una sola jornada.
Objetivos: conocer en qué grado los pacientes con patología digestiva pueden beneficiarse del sistema de consultas en acto único.
Material: estudio descriptivo de 179 episodios de primeras vistas seleccionadas aleatoriamente de una consulta de alta resolución de gastroenterología. Analizamos el porcentaje de pacientes que se beneficiaron de una consulta en acto único así como de las pruebas complementarias realizadas.
Resultados: las patologías más frecuentes atendidas fueron la dispepsia (16%), los antecedentes familiares de cáncer de colon (16%) y enfermedad por reflujo gastroesofágico (16%). Setenta y nueve (44%) de las primeras visitas se resolvieron en consulta única y 80 (45%) de una prueba diagnóstica (100% ecografía abdominal) y revisión tras esta en el mismo día. La realización de una prueba en el día incrementaba significativamente el porcentaje de consulta única frente a los que no se les realizaba (57% frente a 34%, p < 0,002). Los pacientes con enfermedad por reflujo gastroesofágico, dispepsia, colelitiasis y hepatopatía crónica eran las patologías que terminaban en mayor porcentaje en consulta única.
Conclusiones: las consultas de gastroenterología pueden beneficiarse en gran medida de un sistema de consulta de alta resolución solo con cambios organizativos y sin costes adicionales especiales.
Palabras clave: Consulta de alta resolución. Consulta acto único. Consulta de digestivo.
Introduction
Hospital care is increasingly resulting in a predominance of outpatient consultations, which have evolved from a point of care for patients after hospital discharge to become the axis of specialty care activities, a proper place for reaching a diagnosis and establishing a therapeutic strategy. Thus, hospitalization has become a supporting instrument in the diagnostic process, one which is only used when necessary and for the shortest duration possible. Furthermore, the development of bloodless, minimally aggressive diagnostic resources both facilitates and allows ambulatory diagnosis for most medical conditions (1).
More than a decade back our hospital implemented an HRC or single consultation system defined as "an ambulatory process of assistance wherein a diagnosis and treatment are established and recorded all on the same day and with a duration previously agreed upon by the user after being timely informed" (2). The organizational novelty of this system is that patients, once assessed by a specialist during a first visit, may, when appropriate, undergo the indicated diagnostic tests and have them reviewed by that same specialist on the same day. The patient may be then discharged, be scheduled for a follow-up visit or be referred to another department or site.
Complementary tests available in our site that may be performed on a same day basis include all those requiring no prior preparation on the patient's part (CBC, basic biochemistry panel, coagulation testing, gasometry, electrocardiography, ultrasonography, plain radiography, computed tomography, spirometry, etc.). In addition, tests and procedures ordered during the initial visit are processed by ancillary services (mainly in the biotechnology and imaging areas) as preferential activities with a maximum response time of three hours (3).
In the scientific literature the experience with this type of outpatient consultations and their impact on the health care of patients with digestive diseases in our country is very sparse (2,4). These studies suggest that single-day care for outpatients with digestive complaints is below the level observed in other medical specialties (2,4-6). Recently, a multicenter study pointed out which structural and organizational requirements were deemed key by gastroenterologists for such ambulatory consultations (7).
The goal of our study was to analyze the resolution level of a gastroenterology outpatient clinic with the possibility to order and obtain basic examinations for patients on the same day, as well as the conditions that may primarily benefit from HRC.
Patients and Methods
Setting and subjects
Hospital de Montilla is a 77-bed public hospital that serves Montilla (Córdoba, Spain) and its surroundings (5 villages more), which represents a population of 63,742 inhabitants. The hospital is managed by Agencia Pública Empresarial Alto Guadalquivir, a part of Junta de Andalucía (Andalusian government) that includes 7 centers in the Córdoba and Jaén provinces, caring for about 252,000 people. Our gastroenterology outpatient clinic receives a high number of visits, with 302 first visits per 10,000 population during 2014. The hospital runs two gastroenterology offices daily, with approximately 54 first visits weekly. The clinic is tended to by two specialists in gastroenterology and nurses. The hospital has digital medical records with online access to laboratory and diagnostic test results via the Internet. The clinic also has an ultrasound device for abdominal sonography. Study subjects included patients first visiting the gastroenterology clinic at Hospital de Montilla. Regarding sample size, we considered the number of single-consultation visits to be 15% of the 1,900 first gastroenterology visits per year, with a sampling error of 5% and a confidence level of 95%. Thus, we needed at least 177 first-visit patients to characterize the study variables.
Design
This was a descriptive study carried out at our hospital's gastroenterology clinic from October 1st, 2014 to January 31st, 2015. During said period 764 first visits and 138 gastroenterology visits occurred. Patient selection for the study was performed using a random number table. This system selected which patients were eventually studied daily, the physician being beforehand unaware of who was o was not to be recruited.
Variables analyzed
Variables for each visit were recorded by the attending physician following patient care. For each first-visit event a number of variables were recorded using the office computer - age and sex, procedence (primary care, emergency room, referral), patient history (diabetes mellitus, blood hypertension and GI history), test results provided, test performed and reviewed the same day, clinical diagnosis after first visit, destination after first visit (discharge, subsequent visit, referral to another specialist or site), and whether the consultation was considered a single event or otherwise (first visit with clinical report including diagnosis and treatment, regardless of patient destination).
Statistical analysis
Data were analyzed with the statistical software packages ACCESS and SPSS-PC 12.0. Results are expressed as mean (standard deviation) values, assuming an error of 5%. Quantitative variables were studied with Student's t-test. For percent comparisons we used the Chi-squared test. Statistical significance was considered for p < 0.05.
Ethical aspects
The study was approved by the Ethics Committee at Hospital de Montilla (Córdoba, Spain).
Results
We included 179 patients from the 764 first visits that took place during the analysis period. Table I lists the epidemiological and clinical characteristics of recruited patients. Mean age was 54±18 years, with women predominating (53%). Patient origin was mainly primary care (72%) and 76 patients (43%) povided recent routine testing results.
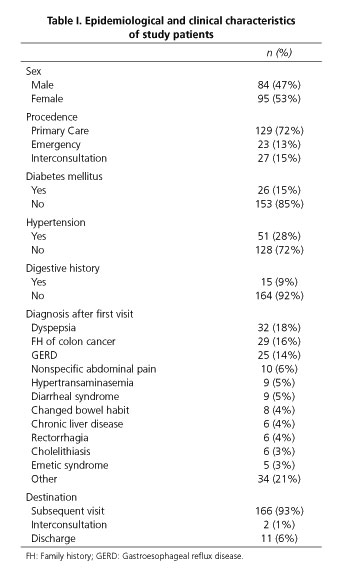
Main diagnoses after a first visit included dyspepsia (16%), a family history of colon cancer (16%) and complaints related to gastroesophageal reflux disease (16%). In all, 72% of patients were scheduled for a subsequent visit, 15% were discharged after their first visit and 13% were referred to a different specialist or hospital.
Seventy-nine (44%) fist visits were solved in a single consultation (patient care where at least one diagnosis and treatment are recorded in a clinical report); 57% of these single consultations (n = 45) benefited from a diagnostic test (100% from GI ultrasounds), which was reviewed on the same day (Table II and Fig. 1). Similarly, 80 patients (45%) among the original 179 patients benefited from same-day testing and review (abdominal ultrasounds). Same-day testing and review significantly increased the percentage of single consultations as compared with its absence (57% versus 34%, p < 0.002). Furthermore, cases benefiting from this system included the younger patients (52.2±19 years versus 57±16 years, p < 0.03).


Of all 79 single-consultation visits, 67 (85%) were followed by a subsequent visit, the remaining subjects being discharged or referred to a different specialist (16%). In contrast, regarding the 100 non-single-consultation visits, 99% of subjects were scheduled for a subsequent visit and 1% were referred to another specialist (p < 0.05) (Fig. 1).
Finally, regarding main complaints, gastroesophageal reflux disease, dyspepsia, cholelithiasis and chronic liver disease were the conditions most commonly ending up in single-consultation care (Table II). Table II illustrates the distribution of conditions in patients undergoing same-day testing, which included GI ultrasounds for 100% of cases.
Discussion
Our results show that gastroenterology consultations may largely benefit from a HRC system, thus being consistent with previous results (2,3). We see, however, that the percentage of patients that may end up with a diagnosis and treatment all in the same day is significantly lower when compared to other specialties (2,4,5). These findings are logical given the characteristics of subjects with digestive complaints, who often need diagnostics tests requiring prior preparation beyond a fasting state (colonoscopy, colon CT, etc.) or laboratory workups that cannot be performed on a same day basis (hepatitis serology, celiac disease testing, etc.).
Although our center offers complementary exams that may be performed on the morning of a first visit, and medical orders are preferentially processed by ancillary services, no patient benefited from such possibilities in our study. We understand that this is, at least partly, a consequence of the significant number of patients who could provide a recent routine laboratory workup during their first visit. This likely reflects our agreements with primary care and our working based on integrated care processes, where patients are referred to our clinic fasting and with recent laboratory results.
We observed it was the presence of a sonography device at the gastroenterology office that allowed a faster diagnosis, consistent with recommendations in this respect (7). However, while many patients were fasting, no upper digestive endoscopy was performed even when applicable. While we initially believed this to be feasible and performed a few such procedures (8), the time-consuming nature of this exploration is not well suited for daily practice.
Furthermore, despite the fact that 44% of our patients benefited from a single-consultation visit, most were scheduled for a subsequent visit on a different day. The reason was that, albeit these subjects had their diagnosis and treatment on the first day, a new follow-up visit was deemed necessary for most of them (condition outcome, response to therapy assessment, delayed laboratory testing results). We therefore understand that the progress brought about by a gastroenterology single-consultation system lies in the potential to perform testing and review the patient on the same day, which shortens diagnostic delay and reduces the number of necessary visits.
Limitations in our study likely include its single-center condition. However, we must here underscore the fact that our high-resolution consultation system has been in place for over 15 years in 7 sites at different hospitals since the begining, with results very similar to those of the present study (2,3).
To conclude, we believe that this kind of consultations represent a clear advance in patient care, with a resolution that relieves delayed diagnosis and treatment, reduces the number of successive visits and increases patient satisfaction (9). This is primarily achieved through organizational changes that do not entail higher costs but do require a high level of involvement by professionals.
References
1. Zambrana García JL. Las consultas ambulatorias de especialidades. Presente y perspectivas de futuro. Med Clin (Barc) 2004;123:257-9. DOI: 10.1157/13065201. [ Links ]
2. Zambrana García JL, Jiménez-Ojeda B, Marín Patón M, et al. La consulta única o de alta resolución como una alternativa de eficiencia a las consultas externas hospitalarias tradicionales. Med Clin (Barc) 2002;118:302-5. DOI: 10.1016/S0025-7753(02)72366-X. [ Links ]
3. Rosa-Jiménez F, Martos Melguizo L, Montijano Cabrera AM, et al. Impacto de los sistemas automatizados en un modelo de consulta de alta resolución. An Med Interna (Madrid) 2005;22:511-4. DOI: 10.4321/S0212-71992005001100002. [ Links ]
4. Puente JJ, Rodríguez FJ, Bernal E, et al. La consulta de alta resolución en aparato digestivo. Rev And Patología Digestiva 2003;26:23-7. [ Links ]
5. Bravo Santervás JM, Zambrana García JL, Ruiz Romero JA, et al. Impacto sobre el tiempo de espera del modelo de consulta única en Neumología frente a la consulta convencional. Neumosur 2002;14: 187-92. [ Links ]
6. Montijano Cabrera AM, Zambrana García JL, Amat Vizcaíno M, et al. Aplicabilidad y aportaciones al sistema de consulta única en cardiología. Rev And Card 2003;38:69-76. [ Links ]
7. Herrerías Gutiérrez JM, Argüelles Arias F, Martín Herrera L, et al. Consulta de alta resolución de digestivo en Andalucía, ¿qué es y cómo debe funcionar? Rev Esp Enferm Dig 2008;100:5-10. DOI: 10.4321/S1130-01082008000100002. [ Links ]
8. Puente Gutiérrez JJ, Rodríguez González FJ, Ramírez Aguilar A, et al. Papel de la endoscopia digestiva alta en un modelo de alta resolución (abstract). Gastroenterol Hepatol 2002;25:170-222. [ Links ]
9. Montijano A, Rosa-Jiménez F, Rubio JM, Monrobel A, et al. Análisis comparativo de la opinión de los pacientes en las consultas de cardiología de dos hospitales de alta resolución. Rev And Cardiol 2005; 40:163-8. [ Links ]
![]() Correspondence:
Correspondence:
José Luis Zambrana-García.
Assistance Coordination Unit.
Hospital de Montilla.
Ctra. Montoro-Puente Genil, km. 65.
14550 Montilla, Córdoba. Spain
e-mail: jlzambrana@ephag.es
Received: 09-06-2015
Accepted: 03-08-2015
