










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.108 no.3 Madrid mar. 2016
LETTERS TO THE EDITOR
Acute transverse colon volvulus with secondary gastric ischemia. Case report
Key words: Transverse volvulus. Colon volvulus. Gastric ischemia. Management.
Dear Editor,
Colonic volvulus occurs when a part of the colon twists over its own mesentery causing intestinal obstruction (1). Approximately 10% of acute intestinal obstructions are secondary to this entity (1,2). Volvulus of the transverse colon is extremely rare (0.2-0.3%) (3) and it was first described by Kallio in 1932 (4). Several anatomical and pathological aspects have been described as risk factors for transverse colon volvulus, some of which are: redundant colon, distant angle flexures with low or absent fixation, chronic constipation, etc. (2,5).
Case report
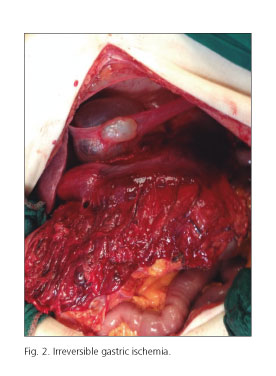
Eighty-one year old patient without relevant medical or surgical history presented with acute abdominal pain and distension. The patient denied any previous similar episodes of abdominal pain and presented with important bloating, tympanic percussion and painful palpation without peritonism in the abdominal exam. Abdominal plain X-ray showed an important dilation of the colon. No pneumoperitoneum was observed (Fig. 1). Colonoscopic devolvulation was then carried out as first therapeutical approach. Present dilation of sigmoid colon was observed. An area of stenosis with congestive and bleeding mucosa was detected proximal to the sigmoid colon. Given the potential risk of perforation and the patient's poor tolerance to the exam, immediate exploratory laparotomy was indicated. A large necrotic volvulated transverse colon that included the gastric body and antrum was found. The stomach presented signs of irreversible ischemia. Important dilation of right side colon was also observed (Fig. 2). In view of these findings, a subtotal colectomy and subtotal gastrectomy was carried out with a Roux-en-Y reconstruction. The patient presented with grade II Clavien-Dindo postoperative complications. Hospital discharge was done on the 13th postoperative day. Anatomopathological study of the surgical specimen revealed the presence of colonic and gastric ischemia (Fig. 3). No signs of malignancy were found in the study. Eight-month follow-up of the patient has shown no signs of malnutrition or intestinal obstruction.


Discussion
Transverse colon volvulus is a rare cause of intestinal obstruction but it represents a surgical emergency (5). Protective factors for the development of this rotation are the hepatic and splenic flexures and the shortness of transverse mesocolon (2,6). Acute abdominal pain, distension and constipation consist of the most frequent clinical trial. The great majority of cases are diagnosed intraoperatively (7). Colonoscopic decompression is not recommended as a treatment for this type of volvulus given the high probability of colonic necrosis (6,8); hence surgery should be the first hand attitude. Simple devolvulation or colopexy are techniques associated with high rates of recurrence, and they are not recommended. The treatment of choice for patients with transverse colon volvulus should be colectomy (5). Decision for immediate or delayed reconstruction is made taking into account the overall status of the patient. In this case, unawareness of the actual diagnosis of the patient prompted the initial colonoscopic approach. The absence of peritonitis and the overall stability of the patient during surgery supported the decision of immediate reconstruction with adequate results.
Ángela Sala-Hernández, Salvador Pous-Serrano,
Elí Lucas-Mera and Nicolás Carvajal-Amaya
Department of General Surgery. Hospital Universitario La Fe. Valencia, Spain
References
1. Codina A, Farres R, Olivet F, et al. Vólvulo de colon y recidiva del vólvulo: ¿qué debemos hacer? Cir Esp 2011;89:237-42. DOI: 10.1016/j.ciresp.2010.12.010. [ Links ]
2. Margolin DA, Whitlow CB. The pathogenesis and etiology of colonic volvulus. Seminars in Colon and Rectal Surgery 1999;10:129-38. [ Links ]
3. Lepage-Saucier M, Tang A, Billiard JS, et al. Small and large bowel volvulus: Clues to early recognition and complications. Eur J Radiol 2010;74:60-5. DOI: 10.1016/j.ejrad.2009.11.010. [ Links ]
4. Sage MJ, Younis J, Schwab KE, et al. Colopexy as treatment option for the management of acute transverse colon volvulus: A case report. J Med Case Rep 2012;6:151. DOI: 10.1186/1752-1947-6-151. [ Links ]
5. Sana L, Ali G, Kallel H, et al. Spontaneous transverse colon volvulus. Pan Afr Med J 2013;14:160. DOI: 10.11604/pamj.2013.14.160.2073. [ Links ]
6. Walczak DA, Czerwińska M, Fałek W, et al. Volvulus of transverse colon as a rare cause of obstruction - A case report and literature review. Pol Przegl Chir 2013;85:605-7. DOI: 10.2478/pjs-2013-0090. [ Links ]
7. Ibáñez S, Borruel N, Cano R, et al. Vólvulos del tracto gastrointestinal. Diagnóstico y correlación entre radiología simple y tomografía computarizada multidetector. Radiology 2015;57:35-43. [ Links ]
8. Echenique M, Amondaraín JA. Colonic volvulus. Rev Esp Enferm Dig 2002;94:201-5. [ Links ]
