










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.108 n.3 Madrid Mar. 2016
LETTERS TO THE EDITOR
Surgical management of appendiceal adenocarcinoid. Case report and literature review
Key words: Adenocarcinoid tumor. Appendiceal neoplasms. Appendicitis.
Dear Editor,
Adenocarcinoid tumor of the appendix is a rare entity characterized by the presence of a double component (neuroendocrine and glandular). It originates in the neuroendocrine cells of the appendicular mucosa. A preoperative diagnosis of a primary appendiceal tumor is uncommon and more so one suggesting an adenocarcinoid pathology.
Case report
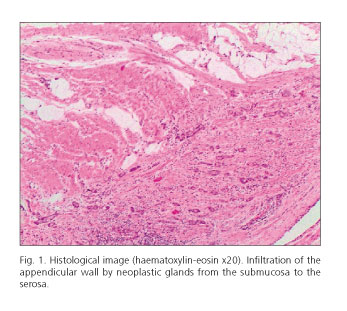
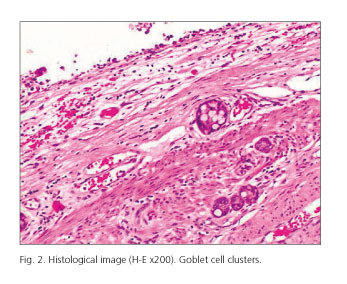
A 57-year-old woman consulted for nausea and abdominal pain in the right hemiabdomen. The patient had no fever or any other clinical data. Ultrasonography and CT informed of a perforated acute appendicitis contained by an inflammatory mass. An emergency laparoscopic appendectomy was performed, revealing a gangrenous acute appendicitis. The pathological report informed of infiltration of the appendicular wall by a primary adenocarcinoid tumor (Figs. 1 and 2). Under this diagnosis a second surgery was performed to extend the resection with a right hemicolectomy. There were no tumor data in the anatomopathological specimen.
Discussion
Appendiceal tumor is an extremely rare entity, accounting for 0.5% of gastrointestinal tract tumors. Garin conducted a review (1) of 7,970 cases of acute appendicitis and found 74 appendiceal tumors (0.9%), including metastatic tumors, and only 2% were adenocarcinoid appendiceal tumors (1).
The mean age at presentation of adenocarcinoid is usually around 50 years (unlike typical carcinoid tumors, which appear around 35- years) with predominance in women (2). The most common presentation is an acute appendicitis although it can also appear as abdominal pain with a palpable abdominal mass. Most cases with this type of presentation tend to be wrongly diagnosed as primary ovarian tumors. Adenocarcinoid has not been reported to cause carcinoid syndrome (3,4).
They are characterized by the presence of two well differentiated histological components: neuroendocrine and glandular (5-7). They are positive, therefore, for endocrine cell staining such as chromogranin A and synaptophysin, as well as for mucin. Unlike carcinoid tumors, the S100 marker is characteristically negative. Despite arising in mucosal crypt cells, the adenocarcinoid tumor characteristically maintains a normal mucosa with submucosa and muscularis propria extension (8).
Tumors are classified according to histological criteria into three groups: group A, typical adenocarcinoid, with well-defined goblet cells arranged in clusters or cohesive linear pattern, with minimal cytologic atypia; group B, adenocarcinoid with signet ring cells arranged in irregular large clusters, with significant cytologic atypia; and group C, poorly differentiated adenocarcinoid with not otherwise distinguishable from a poorly differentiated adenocarcinoma in which there is minimum focal evidence of goblet cells or a confluence of signet ring cells (2).
Due to the infrequency of this pathology and, therefore, to the lack of experience in its management, there is an ongoing debate regarding the correct treatment option (3,6-8). However, the MSKCC pathological classification recommends an appendectomy for type A (typical adenocarcinoid), a right hemicolectomy for type B (signet ring), and a hemicolectomy, hysterectomy and bilateral ovariectomy for type C (poorly differentiated) (2,9).
Localized adenocarcinoid tumors occurred equally in males and females, while disseminated tumors have been seen in females mainly, mostly in the form of a Krukenberg's tumor or peritoneal carcinomatosis, with a very poor prognosis (9).
Elena González-Sánchez-Migallón, Graciela Valero-Navarro, Joaquín Sola-Pérez,
José Andrés García-Marín, María Ángeles Verdú-Fernández, Victoriano Soria-Aledoand
and José Luis Aguayo-Albasini
Department of General Surgery. Hospital Universitario Morales Meseguer.
Campus de Excelencia Internacional "Mare Nostrum". Universidad de Murcia. Murcia, Spain
References
1. Garin L, Corbinais S, Boucher E, et al. Adenocarcinoid of the appendix vermiformis. Complete and persistent remission after chemotherapy (Folfox) of a metastatic case. Dig Dis Sci 2002;47:2760-2. DOI: 10.1023/A:1021065407822. [ Links ]
2. Tang LH, Shia J, Soslow RA, et al. Pathologic classification and clinical behavior of the spectrum of goblet cell carcinoid tumors of the appendix. Am J Surg Pathol 2008;32:1429-43. DOI: 10.1097/PAS.0b013e31817f1816. [ Links ]
3. Bucher P, Gervaz P, Ris F, et al. Surgical treatment of appendiceal adenocarcinoid (goblet cell carcinoid). World J Surg 2005;29:1436-9. DOI: 10.1007/s00268-005-7958-y. [ Links ]
4. Ahmad J, Andrabi SI, Thekkinkattil DK, et al. Adenocarcinoid tumor of the appendix masquerading as acute appendicitis: A word of caution. Ulus Travma Acil Cerrahi Derg 2008;14:167-9. [ Links ]
5. Welsh-Rodríguez J, Arenas-Osuna J, Servín-Torres E, et al. Adenocarcinoid neoplasm of the colon. Case report. Rev Med Inst Mex Seguro Soc 2012;50:441-4. [ Links ]
6. Toumpanakis C, Standish RA, Baishnab E, et al. Goblet cell carcinoid tumors (adenocarcinoid) of the appendix. Dis Colon Rectum 2007;50:315-22. DOI: 10.1007/s10350-006-0762-4. [ Links ]
7. Pahlavan PS, Kanthan R. Goblet cell carcinoid of the appendix. World J Surg Oncol 2005;20:36. [ Links ]
8. Rosai J. Surgical Pathology. 10th ed. New York: Elsevier; 2011. p. 722-4. [ Links ]
9. Olsen IH, Holt N, Langer SW, et al. Goblet cell carcinoids: Characteristics of a Danish cohort of 83 patients. PLoS One 2015;10:e0117627. DOI: 10.1371/journal.pone.0117627. [ Links ]
