










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.108 no.8 Madrid ago. 2016
LETTERS TO THE EDITOR
Intestinal endometriosis. Our experience
Endometriosis intestinal. Nuestra experiencia
Key words: Endometriosis. Bowel endometriosis. Intestinal obstruction.
Palabras clave: Endometriosis. Endometriosis intestinal. Obstrucción intestinal.
Dear Editor,
Intestinal endometriosis, described by Sampson in 1922, is defined as a bowel infiltration by ectopic endometrial tissue (1). The prevalence is 3-37% of all women affected by endometriosis. Rectosigmoid colon is the most frequent location (70-93%), followed by ileocecal region, appendix and other colon and small bowel segments (1-3).
We present 17 cases of patients from our hospital diagnosed with intestinal endometriosis from 2006 to 2015.
Case report
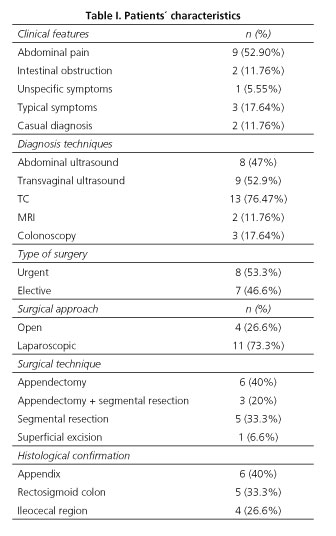
The average age was 35 years old (range 21-53). Three women (17.64%) had previous surgeries for endometriosis. Our patients' features are described in table I. The two patients who did not have surgical treatment received hormonal therapy and following clinic-radiology, with good response. Eight of the patients who had surgical treatment received hormonal therapy. The others refused it. Average follow-up time was 24.82 months (range 60-1). Three of them (17.64%) had a recurrence. One patient received non surgical treatment and clinical follow-up. Surgical treatment was performed in two cases: sigmoidectomy (deep endometriosis) and ileocecal resection (obstruction).
Discussion
Intestinal endometriosis is usually asymptomatic. It is often only diagnosed during surgery for other reasons. Symptoms are frequently nonspecific, with considerable overlap with other clinical gastrointestinal conditions, although it may appear as an acute abdominal pain.
Clinical history, physical examination and image techniques (transvaginal and rectal ultrasonography, TC and MRI) and, sometimes, exploratory laparoscopy are necessary for the diagnosis. Colonoscopy rarely shows mucosal involvement. The definitive diagnosis is the histological confirmation (2,4,5).
The choice of the operative technique depends on the clinical presentation and on the patient's fertility wishes. Laparotomy and laparoscopy are equally effective, but laparoscopic approach is preferred. Segmental resection, discoid excision and superficial shaving are the surgical options, depending on the location and the extent of lesions. Hysterectomy and adnexectomy are indicated if the patient does not wish to conceive (2).
Ángela Sánchez-Cifuentes, María Fe Candel-Arenas and
Antonio Albarracín-Marín-Blázquez
Department of General Surgery and Digestive Diseases.
Hospital General Universitario Reina Sofía. Murcia, Spain
References
1. Durruty G, Larraín de la C. D, Cuello M, et al. Endometriosis profunda del tabique rectovaginal con compromiso intestinal: manejo quirúrgico con resección segmentaria de rectosigmoides. Rev Chil Obstet Ginecol 2008;73:192-203. DOI: 10.4067/S0717-75262008000300009. [ Links ]
2. Bianchi A, Pulido L, Espín F, et al. Endometriosis intestinal. Estado actual. Cir Esp 2007;81:170-6. DOI: 10.1016/S0009-739X(07)71296-4. [ Links ]
3. Milone M, Vignali A, Milone F, et al. Colorectal resection in deep pelvic endometriosis: Surgical technique and post-operative complications. World J Gastroenterol 2015;21:13345-51. DOI: 10.3748/wjg.v21.i47.13345. [ Links ]
4. Ruiz-Tovar J, Pina Hernández JD, Lobo Martínez E, et al. Endometriosis intestinal. Rev Esp Enferm Dig 2007;99:732-3. DOI: 10.4321/S1130-01082007001200013. [ Links ]
5. Ruiz Marín M, Parra Baños PA, González Valverde FM, et al. Appendiceal intussusception resulting from endometriosis presenting as acute appendicitis. Am Surg 2010;76:906-8. [ Links ]
