










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.108 no.9 Madrid sep. 2016
PICTURES IN DIGESTIVE PATHOLOGY
Upper gastrointestinal bleeding in a patient with Sjögren syndrome
Margarida Cortes1, Samuel Raimundo Fernandes2, Vítor Teixeira3 and Luís Carlos Freitas2
Departments of 1Internal Medicine, 2Gastroenterology and Hepatology, and
3Rheumatology. Hospital de Santa Maria. Centro Hospitalar Lisboa Norte. Lisbon, Portugal
Case Report
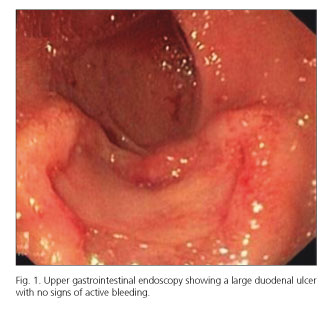
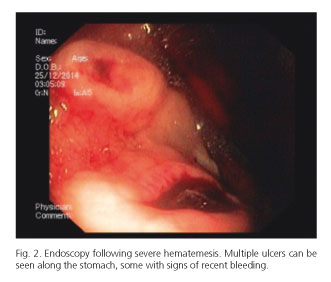
A 68-year-old female was admitted following a 2-month course of asthenia, anorexia and weight loss. She had been diagnosed at age 50 with Sjögren syndrome with articular and glandular involvement. Her medication included prednisolone 5 mg/day. She denied taking off-the-counter medication. An upper gastrointestinal endoscopy (UGE) performed 2 weeks earlier revealed a 15 mm ulcer with raised edges in the duodenum with no signs of active bleeding (Fig. 1) which was biopsied. There were no signs of gastric disease. She was admitted due to worsening of her condition. At admission, her vital signs were normal with unremarkable physical examination. Laboratory tests showed mild normocytic anemia (10.8 g/dl) with raised lactate dehydrogenase (1,852 U/L). On the third day of admission, she developed severe hematemesis with hypotension. Urgent UGE showed multiple gastric and duodenal ulcers, some with active bleeding requiring endoscopic therapy (Fig. 2). Twenty-four hours later, a follow-up endoscopy with biopsies was performed. The two anatomopathological examinations were compatible with gastric and duodenal infiltration by a diffuse CD20+ large B cell lymphoma with germinal center B cell-like morphology. Additional investigation revealed bone, lung, kidney and central nervous system involvement. The patient was referred for chemotherapy with rituximab, cyclophosphamide, doxorubicin, vincristine and prednisolone (R-CHOP) but she unfortunately died one month later due to infectious complications.
Discussion
The risk of lymphoma in Sjögren syndrome is estimated to be 19 to 44 times higher than in general population, rising an average of 7 years after diagnosis. The most common histologic subtypes include MALT and diffuse large B-cell lymphoma. Chemotherapy with R-CHOP remains the mainstay of treatment with survival rates at 3 years of up to 97%.
References
1. Voulgarelis M, Ziakas PD, Papageorgiou A, et al. Prognosis and outcome of non-Hodgkin lymphoma in primary Sjögren syndrome. Medicine (Baltimore) 2012;91:1-9. DOI: 10.1097/MD.0b013e31824125e4. [ Links ]
2. Nocturne G, Mariette X. Sjögren syndrome-associated lymphomas: An update on pathogenesis and management. Br J Haematol 2015;168:317-27. DOI: 10.1111/bjh.13192. [ Links ]
