










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.108 n.10 Madrid Oct. 2016
https://dx.doi.org/10.17235/reed.2016.3939/2015
CASE REPORTS
Conservative management of splenic abscess septic emboli after tooth extractions
Manejo conservador de un absceso esplénico por émbolos sépticos tras extracciones dentarias
Carlos García-Vásquez1, Camilo Castellón-Pavón1, Santos Jiménez-de-los-Galanes1, Juan Gómez-Patiño2 and Belén Brea-de-Diego2
Departments of 1 General Surgery and Digestive Diseases, and
2 Radiology and Vascular Intervention. Hospital Universitario Infanta Elena. Valdemoro, Madrid. Spain
ABSTRACT
Splenic abscesses are rare but may be associated with high mortality. Usually they occur in patients with systemic infection related to some immunocompromised state. The symptoms are nonspecific and the diagnosis is often late, but the development of better imaging techniques has enabled better diagnosis of splenic abscess and percutaneous drainage is a valid and safe complementary treatment option. We report a case of a patient with splenic abscess secondary to septic emboli after tooth extractions, managed conservatively with antibiotics and percutaneous drainage.
Key words: Splenic abscess. Immunosuppression. Splenic preservation. Percutaneous drainage.
RESUMEN
Los abscesos esplénicos son poco frecuentes pero pueden asociar una mortalidad elevada. Generalmente suceden en pacientes con una infección sistémica relacionada con algún estado de compromiso inmunitario. La clínica es inespecífica y el diagnóstico suele ser tardío, aunque el desarrollo de técnicas de imagen más avanzadas ha permitido un mejor diagnóstico de los abscesos esplénicos y disponer del drenaje percutáneo como una opción terapéutica complementaria válida y segura. Presentamos un caso de un paciente con un absceso esplénico por émbolos sépticos tras extracciones dentarias, manejado conservadoramente con antibioticoterapia y drenaje percutáneo.
Palabras clave: Absceso esplénico. Inmunosupresión. Preservación esplénica. Drenaje percutáneo.
Introduction
The splenic abscess is a rare entity with prevalence between 0.14 and 0.7% in autopsy studies (1,2). Usually it is not taken into account in the initial diagnosis of patients with abdominal symptoms and the natural history is associated with a high mortality (1-3). It is usually accompanied by other pathologies that lead to an immunocompromised state (1-3), which together with its vague expressions makes diagnosis and treatment to be delayed. In recent years, the evolution of imaging techniques has helped to improve early diagnosis and develop non-surgical management of these patients (1). We report the case of an 81-year-old patient with a splenic abscess treated conservatively.
Case Report
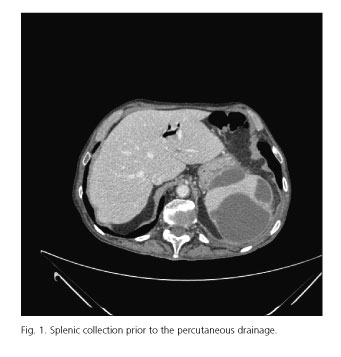
Male, 81-years-old, with a history of chronic obstructive pulmonary disease, hypertension, and chronic renal failure, who is derived from his nursing home because of abdominal pain and fever of 24 hours of evolution. No clear history of trauma, but he refers multiple tooth extractions, the latter two carried out a week and 24 hours before the onset of symptoms. Upon arrival at the emergency room the patient presents no fever, with cough and expectoration. The physical examination revealed a septic mouth, bilateral rhonchi and diffuse abdominal pain without signs of peritoneal irritation. In the initial analysis, no leucocytosis or formula alteration was found, with haemoglobin of 11 g/dl and haematocrit of 36.5%. In the basic chest X-ray minimal bilateral pleural effusion without pulmonary infiltrates are seen. Within 24 hours, the patient experiences a general deterioration, more abdominal pain accompanied by voluntary defence in the left abdomen, leucocytosis (11,600 with 91.1% neutrophils), and anaemia (haemoglobin 8.9 g/dl). A computed tomography (CT) scan is performed, without contrast due to the deterioration of renal function (creatinine 2.1 mg/dl), with a normal spleen size, with heterogeneous density with a peripheral rim sub capsular areas of lower density and lower density within the splenic parenchyma, suggestive of a splenic infarction, the remainder being normal. Given these findings and after recovery of renal function with aggressive fluid therapy, repeated CT with contrast confirms the presence of irregular spleen without contrast enhancement areas compatible with areas of infarction or splenic laceration (Fig. 1), no extravasation of contrast. Conservative treatment was established with antibiotics and analgesia with respiratory symptoms improvement, but persistent abdominal pain, leucocytosis and elevated acute phase reactants. Control CT reveals a splenic subcapsular collection shown in the upper pole of 9 x 11 x 9.5 cm with attenuation values suggestive of haematoma (Fig. 2), so we decided to perform a percutaneous drainage of the splenic yielding to collection of abundant purulent material. In this material, it grows on crops E. coli only sensitive to carbapemenes, so an imipenem cycle is started and percutaneous drainage is maintained with progressive improvement of the general conditions of the patient and laboratory parameters. After 10 days of drainage and in the absence of new debit, a new control abdominal ultrasound is done, checking the disappearance of the collection, so the catheter is removed and the patient is discharged. After 7 months of follow-up, the patient remains asymptomatic, and CT scan shows a normal spleen without intra-abdominal collections.

Discussion
The splenic abscess is a rare infection, with a prevalence of 0.14 to 0.7% in autopsy studies (1,2), but with a high mortality (13-25%) (1-3). The most important predisposing factor is the systemic infection, usually by haematogenous spread of septic emboli from a bacterial endocarditis (68-73%) or another distant septic focus, although they have also been described due to contiguity extension, haemoglobinopathies or after a splenic trauma (3,4). Usually patients with splenic abscess are adult males who have some associated risk factor: immunocompromised states, diabetes mellitus or intravenous drug abuse (1,4). The increment in the amount of immunocompromised patients and the development of better diagnostic imaging techniques have led to an increased incidence of splenic abscesses in the past decades (1-3,5).
The diagnosis of splenic abscess is usually delayed due to its nonspecific clinical characteristic, usually left upper quadrant pain and fever with or without palpable splenomegaly. Leucocytosis is common (78%) and chest radiography may present a left pleural effusion (32-39%) (1,4). The imaging test of choice is abdominal CT, showing a hypodense area of peripheral enhancement after contrast administration. Sometimes it can be difficult to differentiate from a splenic infarction or splenic haematoma, as it happened initially in our case. On ultrasound, splenic abscesses manifest as irregular hypoechoic or anechoic lesions (3,4). Multiple abscesses are less common (31-38%) and less symptomatic but they have a worse prognosis for the increased risk of sepsis (3).
The most commonly isolated pathogens are aerobic gram-positive microorganisms (streptococci and staphylococci) and gram-negative (Klebsiella, E. coli and pseudomonas) (3-5). They are less common anaerobic bacteria or fungi.
Classically the treatment of splenic abscess was a splenectomy (1) and antimicrobial therapy. In recent years, it has been successfully developed a more conservative approach, trying to preserve the organ through an aggressive antimicrobial therapy and radiological guided percutaneous drainage in hemodynamically stable younger patients with unique abscesses, without walls and away from the splenic hilum and in patients with high surgical risk, associated comorbidity, important or serious deterioration of the general status due to the sepsis status (1,3-5). Percutaneous drainage allows choosing the most appropriate antibiotic, avoids the risk of purulent peritoneal dissemination and potential complications of splenectomy, reduces hospital stay, it is better tolerated by the patient and the cost is minor (4,5). However, percutaneous drainage is not without complications and failure rate is high in various series (from 14.3 to 75%) (4,5). Open or laparoscopic splenectomy should be reserved for patients who do not respond to initial medical or interventional treatment or when multiple, multiloculated or recurrent abscesses (1,2,4). In a series of 18 patients with splenic abscess, Lee et al. related the prognosis to the underlying general situation of the patient without appreciating significant differences in mortality among patients treated conservatively and patients undergoing surgery (2).
In our case there was a history of chronic obstructive pulmonary disease and chronic kidney disease with a known septic focus (mouth) as outstanding and potential source of septic emboli. The treatment of splenic abscess is controversial and must be individualized. Although some authors recommend percutaneous drainage of abscess under 3 cc (6), the favourable response in this case supports the validity and safety of this therapeutic alternative even in larger abscesses.
References
1. Liu YH, Liu CP, Lee CM. Splenic abscesses at a tertiary medical center in northern Taiwan. J Microbiol Immunol Infect 2014;47:104-8. DOI: 10.1016/j.jmii.2012.08.027. [ Links ]
2. Lee WS, Choi ST, Kim KK. Splenic abscess: A single institution study and review of the literature. Yonsei Med J 2011;52:288-92 DOI: 10.3349/ymj.2011.52.2.288. [ Links ]
3. Iñíguez A, Butte JM, Zuñiga JM, et al. Abscesos esplénicos. Comunicación de siete casos y revisión de la literatura. Rev Med Chile 2008;136:38-43. DOI: 10.4067/S0034-98872008000100005. [ Links ]
4. Sreekar H, Saraf V, Pangi AC, et al. A retrospective study of 75 cases of splenic abscess. Indian J Surg 2011;73:398-402. DOI: 10.1007/s12262-011-0370-y. [ Links ]
5. Ferraioli G, Brunetti E, Gulizia R, et al. Management of splenic abscess: Report on 16 cases from a single center. Int J Infect Dis 2009;13:524-30. DOI: 10.1016/j.ijid.2008.08.024. [ Links ]
6. Jaiswal CSS, Talreja LCM, Chawla SLB, et al. Organ preservation in splenic abscess. Med J Armed Forces India 2014;70:195-7. DOI: 10.1016/j.mjafi.2012.06.008. [ Links ]
![]() Correspondence:
Correspondence:
Carlos García-Vásquez.
Department of General Surgery and Digestive Diseases.
Hospital Universitario Infanta Elena.
Av. Reyes Católicos, 21.
28342 Valdemoro. Madrid, Spain.
e-mail: cgv1@hotmail.com,
cgarciava@idcsalud.es
Received: 24-07-2016.
Accepted: 31-07-2016
