










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 n.2 Madrid Feb. 2017
https://dx.doi.org/10.17235/reed.2016.4441/2016
ORIGINAL PAPERS
Practical aspects of high resolution esophageal manometry
Aspectos prácticos para la manometría esofágica de alta resolución
Antonio Ruiz-de-León-San-Juan1, Constanza Ciriza-de-los-Ríos2, Julio Pérez-de-la-Serna-Bueno1, Fernando Canga-Rodríguez-Valcárcel2, Fermín Estremera-Arévalo3, Raquel García-Sánchez4, Jose Walter Huamán-Ríos5, María Teresa Pérez-Fernández6, Cecilio Santander-Vaquero6, Jordi Serra-Pueyo7, Concepción Sevilla-Mantilla1, Elisabeth Barba-Orozco8, María José Bosque-López9, Sergio Casabona-Francés6, Silvia Carrión-Bolorino10, Pilar Castillo-Grau11, Silvia Delgado-Aros12, Ana Belén Domínguez-Carbajo13, Pilar Fernández-Orcajo14, Javier García-Lledó15, Froilán Gigantó-Tomé16, Rosa Iglesias-Picazo3, Gloria Lacima-Vidal17, Pilar López-López18, Magdalena Llabrés-Rosselló9, Pilar Mas-Mercader19, Marianela Mego-Silva8, María Usua Mendarte-Barrenetxea19, Carlos Miliani-Molina20, Milagros Oreja-Arrayago3, Francisco Sánchez-Ceballos1 and Sandra Sánchez- Prudencio21
1Hospital Clínico San Carlos. Madrid, Spain.
2Hospital Universitario 12 de Octubre. Madrid, Spain.
3Complejo Hospitalario de Navarra. Pamplona, Navarra. Spain.
4Hospital Sanitas La Moraleja. Madrid, Spain.
5Hospital General de Catalunya. Sant Cugat del Vallès, Barcelona. Spain.
6Hospital de La Princesa. Madrid, Spain.
7Hospital Germans Trias i Pujol. Barcelona, Spain.
8Hospital Vall d'Hebron. Barcelona, Spain.
9Hospital Universitario Son Espases. Palma de Mallorca, Spain.
10Hospital de Mataró. Barcelona, Spain.
11Hospital Universitario La Paz. Madrid, Spain.
12Hospital del Mar. Barcelona, Spain.
13Complejo Hospitalario de León. León, Spain.
14Hospital Río Hortega. Valladolid, Spain.
15Hospital General Universitario Gregorio Marañón. Madrid, Spain.
16Hospital Universitario Central de Asturias. Oviedo, Spain.
17Hospital Clinic. Barcelona, Spain.
18Hospital Universitario Donostia. Donostia, Guipúzcoa. Spain.
19Hospital Clínico Universitario. Valencia, Spain.
20Hospital Sur Alcorcón/Clínica La Luz. Alcorcón, Madrid. Spain.
21Infanta Cristina. Parla, Madrid. Spain
Conflict of interests: The consensus meeting was sponsored by Covidien, Medtronic, Given Imaging and Synmed.
ABSTRACT
High resolution esophageal manometry (HRM) is currently under development as can be seen in the various Chicago classifications. In order to standardize criteria in certain practical aspects with limited scientific evidence, the First National Meeting for Consensus in High Resolution Manometry of the Spanish Digestive Motility Group took place, bringing together a wide group of experts. The proposals were based on a prior survey composed of 47 questions, an exhaustive review of the available literature and the experience of the participants. Methodological aspects relating to the poorly defined analysis criteria of certain new high resolution parameters were discussed, as well as other issues previously overlooked such as spontaneous activity or secondary waves. Final conclusions were drawn with practical applications.
Key words: High resolution esophageal manometry. Consensus meeting. Spanish Digestive Motility Group.
RESUMEN
La manometría esofágica de alta resolución (MAR) está en fase de desarrollo, como se evidencia por las diferentes clasificaciones de Chicago. Con el fin de unificar criterios en algunos aspectos prácticos con limitada evidencia científica se llevó a cabo la Primera Reunión Nacional de Consenso en Manometría de Alta Resolución del Grupo Español de Motilidad Digestiva, en la que participaron un amplio grupo de expertos. Las propuestas se basaron en una encuesta previa con 47 preguntas, la exhaustiva revisión de la bibliografía disponible y la experiencia de los participantes. Se plantearon aspectos metodológicos sobre criterios de análisis poco definidos de algunos nuevos parámetros de alta resolución y otros aspectos no considerados, como la actividad espontánea o las ondas secundarias, elaborándose conclusiones finales con utilidad práctica.
Palabras clave: Manometría esofágica de alta resolución. Reunión de consenso. Grupo Español de Motilidad Digestiva.
Introduction
Since esophageal manometry was introduced into clinical practice in the mid-70s, technical and methodological changes have taken place that require standardization and a common set of reference values and analysis criteria between laboratories. High resolution esophageal manometry (HRM) has led to advances in the diagnosis and treatment of esophageal motor disorders (1,2). Its incorporation was led by the International High Resolution Manometry Working Group, and provided an opportunity for updating and harmonizing concepts and criteria. The different versions of the Chicago Classification (CCH) which this group created were a significant advance; however, the latest version (3) is incomplete, failing to describe over 30% of patients with manometric findings (4).
Furthermore, the results depend on technical factors: perfusion or micro-driver systems, catheter characteristics, system sensitivity, and probably the software used; and methodological factors: the patient's position, volume and consistency of the bolus, measuring points and parameters used for analysis. The job of improving the harmonization of the techniques and analysis criteria is something that only specialists in the field can and should perform. To this end, the First National Meeting for Consensus in High Resolution Manometry of the Spanish Digestive Motility Group (GEMD) took place on the 7th and 8th of May 2015, the results of which are presented in this article.
The aims of this study were to contribute to the knowledge of the methodology used in this area, to guide and make recommendations on poorly defined and/or controversial aspects and to harmonize the analysis criteria and procedures as far as possible.
Material and methods
The meeting was attended by 30 specialists from 24 motility units with extensive experience. The number of manometries performed each year by all participants was estimated at between 10,000 and 12,000. During the previous months, a survey was conducted with participants with 47 questions designed to evaluate the following: the characteristics of the participating groups, technical and/or methodological aspects and theoretical/practical concepts. The meeting was organized with seven round tables, and the topics and presentations were selected on the basis of the survey results and a review of the published literature (PubMed). The questions selected were those of the most practical interest and on issues with little or no published scientific evidence. Depending on the issues, and where possible, the round tables were supplemented with case studies provided by the participants.
Results and discussion
Should some form of topical anesthesia be used?
Fifty per cent of respondents did not use anesthesia to perform HRM; 20% used aerosol lidocaine and 30% used lidocaine gel.
Current situation
The use of topical anesthetics is optional (5). There are no well-designed multicenter studies to assess their impact on manometry records. The information available suggests that its use does not alter the motor activity of the esophagus, although it could alter the dynamics of the early stages of swallowing (6). Both lidocaine and benzocaine are useful to reduce the discomfort caused by catheterization (7,8). It is recommended that their use be specified in the final report (9).
Conclusions
It is agreed that the use of topical anesthetics:
- Is not essential.
- The existence of possible allergies should be assessed, and the gel should be used for nasal access and the aerosol for oral access.
- This should be specified in the report.
Should usual medication be withdrawn in studies or should studies reflect the medication taken by the patient?
Forty per cent of respondents felt that any medication that could alter esophageal motor activity should be withdrawn; 35% felt it should only be removed for specific studies; 15% felt that only medication that is "not essential" to the patient should be withdrawn; and 10% thought that no medication should be withdrawn.
Current situation
The HRM protocol recommends fasting for six hours and withdrawal of any medication that might alter normal esophageal function at least 24-48 hours before the examination. However, in some circumstances, although the action of a drug is known to affect esophageal motility, this drug may be essential for the patient and therefore withdrawing or maintaining it could alter the final interpretation of the study. The length of time that the treatment should be suspended in order to eliminate the effect of a drug on esophageal motility has not been established, as it varies according to the type of drug.
In studies with protocols that aim to assess motor impairment related to certain pathologies, any medication that could alter the contractile capacity of the esophagus should be withdrawn. This would not be necessary in normal clinical studies.
Some of the most important drugs that can in some way alter esophageal motility are included in table I (10-23).
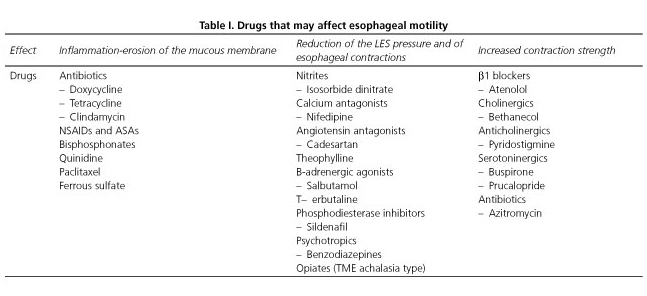
On the other hand, there is no evidence that it is useful to perform examinations with or without medication, although it may be relevant and improve therapeutic management in certain processes. However, if the usual medication is maintained we recommend that this be specified in the report; and if any medication is withdrawn, this should be recorded and the time of withdrawal should be specified.
Conclusions
- In studies specifically designed to detect esophageal motor disorders, any medication that could alter the contractile capacity of the esophagus should be withdrawn.
- Some drugs can cause changes in esophageal motility but no studies have shown that it is useful to perform examinations in "ON" or "OFF".
- Studies that include the "ON-OFF" effect could provide relevant data and improve diagnostic and/or therapeutic management.
- If variations occur in diagnosis, it should be specified in the reports that they may have been caused by medication.
What interval should be maintained between swallows?
Sixty per cent of those surveyed thought that the interval should be at least of ten seconds; 25% advocated for 30 seconds or more, and 15%, as soon as the LES reaches it basal value.
Current situation
In the lower 2/3 of the esophageal body (esophagus made of smooth muscle fiber), the peristaltic contraction is followed by a period of refractoriness during which the esophageal muscle does not respond to excitatory stimuli (24). Swallows performed at intervals of < 10 to 15 seconds can cause an inhibition of the contraction response (5,24,25). Intervals above these limits are recommended. Some protocols recommend 20 seconds (27); others, which include the HRM standard in the CCH, establish periods of 30 seconds (26,28). It is important to note that the greater the interval between swallows, the greater the risk that "spontaneous" anti-protocol swallows occur.
Conclusions
- A ≥ 20 seconds minimum time or interval between liquid swallows is generally sufficient, providing that the contraction activity triggered by the previous swallow has disappeared.
Should a survey be conducted prior to the HRM study? Is a unified protocol required for data collection?
All respondents believed that a survey should be conducted to assess clinical aspects. Fifty-five per cent believed it should be supervised by the physician, 30% believed it should be supervised by the nurse and 15%, that it should only be conducted in special cases or for specific studies.
Regarding the need for a unified protocol, 65% thought that the survey should be unified and common at a national level, 30% thought it was required only for very specific studies and 5% considered it as unnecessary.
Current situation
Data collection prior to manometry studies is not performed according to an agreed protocol. Each group uses their own protocol, often designed for a specific pathology (GERD, dysphagia, chest pain, etc.). The general surveys are often sent alongside rules for preparing the study and vary greatly in their content. No well-structured articles have been found for the specific study of this subject.
Conclusions
- Surveys for evaluating symptoms should be conducted prior to manometry studies, as they provide information that simplifies data collection and analysis.
Should the landmark resting pressures of the sphincters be recorded at the beginning, during the study, or at the end?
Fifty per cent of respondents said that it should be sometimes be done at the beginning and sometimes at the end, depending on the patient's collaboration. 30% said it should be recorded at the beginning, 15% at the end, and 5% wanted an average of various measurements.
Current situation
In some programs it is essential for a reference point for the resting pressures of both sphincters (landmark) to be taken at baseline. These pressures, and particularly that of the upper esophageal sphincter (UES), vary significantly throughout the recorded procedure. Some authors (29) suggest that the values obtained at the end of the test may better reflect its clinical utility.
Conclusions
- Although it is recommended that the reference points are recorded at baseline, in certain cases this should be carried out during or at the end of the procedure, especially in patients with poor initial tolerance.
Should reference be taken on gastric or atmospheric pressure? (Multiple answers)
Twenty per cent of respondents felt that the reference value to assess the resting pressure of the lower sphincter should be gastric pressure in the lowest channel; another 20% opted for the average pressure of all gastric channels; and 5%, for the gastric pressure in the highest channel. Thirty-five per cent thought that atmospheric pressure should be used as a reference.
Current situation
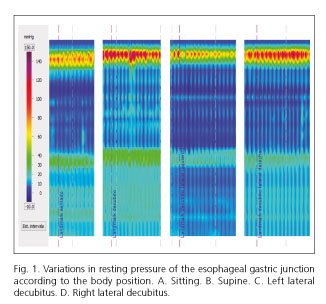
Although atmospheric pressure (AP) is considered to be more accurate and reliable (30), most studies use intra-gastric pressure as a reference. This is due to the technical limitations of perfusion systems (30). Besides, the CCH uses AP for all pressure measurements except for integrated relaxation pressure (IRP), which is referenced to gastric pressure (31). While this approach is justified in that it better reflects the resistance of the bolus during its transit through the esophagogastric junction (EGJ), it is much less useful when certain sensors cannot be placed in the gastric cavity of patients with large hiatal hernias, anti-reflux surgery or after some bariatric surgery techniques (Fig. 1).
Conclusions
- In HRM both pressures, atmospheric and gastric, are used as a zero reference; changes in the reference points would require a broad international consensus.
Are there significant differences between the various analysis systems and programs? (Multiple answers)
Fifty per cent of respondents felt that there were differences between infusion equipment and microtransducers, 40% felt that the catheters had different characteristics, another 40% pointed to differences in software, and 15% found no differences.
Variations of normal values are described in relation to demographic factors (age, obesity, etc.), and technical ones (diameter of the catheter, position of the patient, consistency of the bolus, etc.) (32-36). In addition, the analysis programs are not compatible and the elements of analysis cannot be superimposed. For example, the relaxation of the lower esophageal sphincter (LES) by IRP varies according to the equipment used and to aspects related to the analytical system (e-sleeve).
Conclusions
- It is advisable to have normal values for each HRM system and protocols suited to the characteristics of each piece of equipment. The data should be exportable and compatible with different analysis programs.
Should the study be conducted in different positions and/or with different boluses or textures?
With regard to the necessity of performing studies in different positions, 60% of respondents considered them as necessary only in specific studies; 35%, only exceptionally; for a 10% they were not necessary, and 5% believed they should always be done in the supine and sitting position. As for swallows with different boluses and textures, 75% of respondents felt they were only required in protocols or specific studies and for a 25% they were necessary in patients with dysphagia.
Current situation
The standard HRM protocol is designed for a patient in a recumbent position and with liquid swallows (3,37,38). However, advantages have been identified in certain situations with the patient sitting (39) and using a solid bolus or standardized food (40-42). Although some studies have been published with reference values under these conditions (43,44), such conditions are not common and are not covered by the CCH, which is most commonly used to define esophageal motor disorders (3,31). The fact that the reference values vary significantly depending on the position (recumbent/sitting) at rest (Fig. 1) and on crucial parameters such as the IRP-4s or the distal contractile integral (DCI) (44) raises further doubts about its practical use.
Conclusions
- Currently, HRM studies are standardized for recumbent position and liquid swallows. For the time being it is recommended that this system be maintained.
- It may be useful, especially in patients with dysphagia, to complete studies with swallows in more physiological positions and with different textures.
How much importance should be given to transient relaxations?
Sixty-five per cent of respondents believed that if they occur, they should be specified in the report, 15% considered that their presence indicates an increased likelihood of GER, and another 15% thought that they should only be reported if they were very intense or frequent.
Current situation
Transient lower esophageal sphincter relaxations (tLESRs) are accompanied by esophageal longitudinal muscle contraction and relaxation of the crural diaphragm. They are usually caused by gastric distention and are mediated by a vagal reflex. They occur at a frequency of about 3-6/h. They are considered as a physiological phenomenon that allows gastric gas to be released through eructation (45).
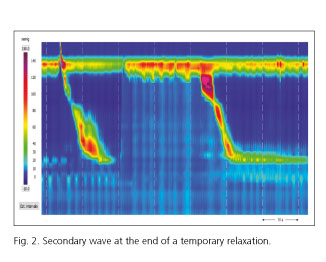
TLESRs are responsible for 64-74% of GER episodes (46,47). Characteristically, TLESRs with longer duration, lower nadir pressure, more diaphragmatic inhibition and ending with a secondary wave are those accompanied by reflux (48) (Fig. 2).
GER episodes associated with tLESRs occur more frequently in standing or right lateral recumbent position, and in obese patients (49). The main determinant of GERD is an increased proportion of tLESRs associated with acid reflux and a higher gastro-esophageal pressure gradient before and during tLESRs than in healthy subjects (45,50).
Conclusions
- The presence of reflux during tLESRs is not always easy to identify if combined studies with impedanciometry were not performed.
- No data are available to set normal limits on the number and characteristics of tLESRs during a conventional study. It would be interesting to know the averages and characteristics of tLESRs that appear in diagnostic studies and their relationship with clinical practice, esophageal pH monitoring and endoscopy.
In patients with a hiatal hernia ≤ 4 cm, where should the LES and gastric pressure sensors be placed? (Multiple answers)
Fifty per cent of respondents felt that the pressure sensors should be placed above and below the high pressure zone, including the crural diaphragm (CD); 35% would place them above and below the high pressure area of the LES excluding the DC, and 25% considered LES and CD should be measured separately, specifying both results. Regarding the gastric sensor, 60% believed it should be placed outside of the hiatal hernia (HH) in the stomach and 15%, within the HH.
In patients with a hiatal hernia > 4 cm, where should the LES and gastric pressure sensors be placed? (Multiple answers)
Thirty per cent of respondents considered that the LES pressure sensors should be placed above and below the high pressure zone of the LES excluding the DC; 35% preferred above and below the high pressure area of the LES including the DC; and 30% recommended separate measurements for LES and CD if the latter is passed, and specifying the results. Regarding the gastric sensor, 60% felt that if the diaphragm had not been passed, the gastric sensor would remain intra hernia and the reference should be AP, or it should be specified that the analysis is made with reference to intra hernial pressure. According to a 10% of respondents, the sensor should be placed within the hiatal hernia, and a 30% would place it outside it.
Current situation
It is believed that the pressure of the EGJ as a whole depends on the LES and CD pressures, which helps to increase the pressure especially on inspiration (51). Under normal circumstances, the esophagus is attached to the diaphragm by the phreno-esophageal membrane, a key structure in the pathogenesis of HH (52-54). From a manometric point of view, three subtypes of EGJ have been described according to their morphology: subtype I (LES and overlapping DC), subtype II (separation between the LES and CD < 2 cm), and subtype III or hiatal hernia (separation between EGJ and CD > 2 cm). This latter subtype is in turn subdivided into IIIa and IIIb (55). The degree of disruption of the EGJ influences the pattern of GER (56). Moreover, the EGJ is a dynamic structure that changes depending on the position of the body, the state of rest or swallowing and breathing movements; thus, when the HH is reduced, fewer episodes of GER occur, and these are caused by tLESRs; however, when it is not reduced, other mechanisms such as relaxation induced by swallowing or hypotonia of the LES become more important (57).
Regarding the metric designed to assess the competence of the EGJ, different values of normal resting pressure have been published, considering the median expiratory and inspiratory pressure, and they vary depending on the type of equipment and catheter used (3). Other possible parameters are being evaluated such as inspiratory increase (55), integral LES pressure (58), the contractile integral of the EGJ (59) and the valuation of intragastric pressure (60).
The published normality limits are so broad that they do not help to distinguish between normal subjects and patients with EGJ dysfunction, so more studies are required to determine the usefulness of the new proposed parameters.
Conclusions
- It is recommended that the morphology of the EGJ be described by defining its subtypes.
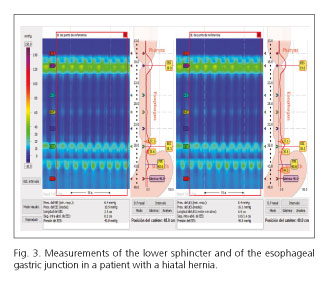
- The HH should be measured. If the abdominal cavity can be passed, there is a consensus on measuring the pressure of the whole EGJ and of the LES, separately (Fig. 3).
- In cases where the HH is very large and the abdominal cavity cannot be passed, pressure should be referenced to AP or intrahernia (specifying in the report that it was not possible to pass the abdominal cavity as well as the reference point taken).
- Although the new metric for EGJ pressure may be promising, there is insufficient evidence for its routine use in clinical practice, thus for now it seems reasonable to continue using the "classical" criteria.
- It is considered as important to specify, if applicable, the existence of compartmentalization between the sphincter and the diaphragm in patients with HH.
Should the cutoff value for the integrated relaxation pressure (IRP) be fixed or adjusted according to the pattern of esophageal contractility?
Fifty-five of respondents considered that it could vary depending on the equipment, the position and on whether the patients had been operated on; 15% thought it should be a fixed value; another 15% deemed it as depended on the system used, and 5% thought it should be adjusted to the pattern of esophageal contractility.
Current situation
The IRP reports the lowest average relaxation pressure, which is determined by using an e-sleeve for four seconds (either continuous or non-continuous) within a window of ten seconds. Initially, the normal value was established as IRP-4s < 15 mmHg with solid state equipment (61). Subsequent studies suggest that a cutoff of ≤ 10 mmHg has greater clinical utility (62,63). In any case, this value should be adjusted according to the pattern of esophageal contractility, the patient's position, whether the patient has been operated on, the equipment used (perfusion systems or solid state) and aspects related to the method of analysis (e-sleeve) (3,53,64-67).
Conclusions
- The IRP must be adjusted according to the equipment used, the patient's position, previous surgery on the EGJ and the pattern of esophageal contractility.
What importance should be given to esophageal shortening? (More than one answer)
Thirty-five percent of respondents felt that the esophageal shortening is more common in patients with motor impairment, 15% felt that it should only be specified if the episodes are particularly severe or frequent and 65% said that they should be reported whenever they occur.
Current situation
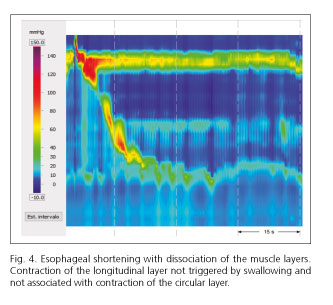
Coordination between the longitudinal and circular muscle is the basis of the pathophysiology of motor disorders (Fig. 4). One of the most interesting contributions of HRM has been its emphasis on the contractile activity of the longitudinal muscle layer identified by esophageal shortening. This technique allows the degree of EGJ sliding to be measured, a better assessment of the coordination between the two muscle layers and a better characterization of the function of the longitudinal muscle (68).
In healthy patients, the mechanism that produces most GER episodes is tLESR (69). There is controversy over whether the phenomenon of esophageal shortening precedes the tLESR, helping to "un-anchor" the LES, or occurs later (70,71). The contraction of the longitudinal muscle during the tLESR produces esophageal shortenings of between 4.3 and 8 cm, while the shortening of swallowing does not exceed 1.8 cm (72).
The latest evidence postulates that the differences between patients with or without GERD depend on the number of tLESRs accompanied by reflux (73). Thus, when the esophageal shortening is > 3 cm, 100% of tLESRs are accompanied by reflux (45). It therefore appears that esophageal shortenings play a key role in GERD.
In patients with a hypercontractile esophagus, dissociation has been observed at the beginning of the contraction of both muscle layers, causing dysphagia by trapping the bolus (68).
The pattern of longitudinal muscle contraction has been associated with the manometric subtypes of achalasia (74): in type I, no contraction occurs; in type II, the contraction is responsible for pan-esophageal pressurization; and in type III, the contraction is not coordinated with the circular layer.
Hypoperfusion of the esophageal wall during longitudinal muscle contraction has been associated with chest pain and treatment-resistant heartburn, by pain related to smooth muscle ischemia (75). Some studies suggest that mild pharyngeal stimuli may cause contraction of the proximal longitudinal muscle, which in turn has been associated with increased tLESRs (76).
Conclusions
- The ability to identify esophageal shortening is a breakthrough in our physiological understanding of GERD and of motor disorders, and in the future it may be a target for new treatments. It seems reasonable that they be reported if they occur during the study.
What is the significance of different aspects of hypercontractile/jackhammer esophagus? (More than one answer)
Seventy-five percent of respondents considered that it is only pathologically significant if the DCI is > 8,000 mmHg cm-1/s-1. Sixty per cent said it does not always occur after swallowing, 45% thought it was not always associated with symptoms, and 10% considered that it is not possible to determine the limit of the upper edge of the EGJ.
Current situation
Jackhammer or hypercontractile peristalsis is an esophageal motility disorder characterized by long duration spastic contractions and involving most of the smooth fiber esophagus. In HRM it is defined as a DCI of over 8,000 mmHg cm-1/s-1 in ≥ 20% of swallows, alongside a normal distal latency and an LES that relaxes normally (3) (Fig. 5). This disorder has not been described in healthy controls, although the patients affected by it not always present with symptoms. Some authors suggest that there is not yet sufficient evidence available to definitively set the limit value above 8,000 mmHg cm-1/s-1 (77).

Conclusions
- There is not sufficient evidence available to definitively set the upper DCI diagnostic limit at 8,000 mmHg cm-1/s-1.
- In some cases it is difficult to differentiate the S3 and S4 esophageal segments during contraction, especially if they are associated with esophageal shortening.
- One option is to include global contractility (S2, S3 and S4) or to establish a theoretical limit by locating the upper border 3 cm above the lower border of the UEG.
Should the basal esophageal pressure be assessed?
Forty per cent of respondents felt that it should always be evaluated; another 40% considered it should be evaluated when relevant, as in achalasia, and 25% would only evaluate it when associated with retention symptoms.
Current situation
In conventional manometry, basal esophageal pressure has been considered to be a useful parameter in the diagnosis of achalasia (78,79). Various criteria have been used for its analysis, and the most common one consists in measuring the nadir of expiration at rest. Its normal value is negative with respect to the gastric expiratory pressure and may vary, increasing throughout the study when the swallowed water is retained in the esophageal body (e.g., achalasia). No limit values have been established, but it is considered to be pathological when equal to or above gastric pressure.
Conclusions
- In HRM the baseline esophageal pressure has not been included among the parameters used in the CCH; however, this information is of great interest as it evaluates retention in the esophageal body. When it is abnormal it should be described in the report.
What is the significance of double-peak and multi-peak waves? (More than one answer)
Forty-five per cent of respondents believed that the presence of waves with three or more peaks was associated with motor disorder, another 45% felt multi-peak waves are always important when they are also simultaneous, and 10% considered them as irrelevant.
Current situation
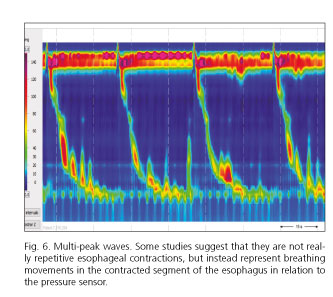
Double peak waves generally occur in the lower esophagus and indicate a delay in the onset of contraction of contractile segment S3 compared to S2. They have no clear pathological significance, but they may suggest the presence of hyper-contractile disorders (80,81). The appearance of waves with three or more peaks (multi-peak waves) is usually associated with an esophageal motor disorder (81). There are no studies to support their clinical relevance as an isolated motor impairment. Some studies suggest that they are not in fact repetitive esophageal contractions, but instead represent respiration movements in the contracted segment of the esophagus in relation to the pressure sensor (82) (Fig. 6). These findings have not been corroborated by subsequent studies (83,84).
Conclusions
- Multi-peak waves are usually associated with an esophageal motor disorder, although their association with an isolated motor impairment has not been demonstrated.
How should simultaneous repetitive contractions be assessed?
Forty-five per cent felt that their presence should be reported but without influencing the assessment of other waves, 15% deemed them as equivalent to a multi-peak wave, and 5% considered that they should not be taken into account.
Current situation
Repeated simultaneous contractions are pathological and their occurrence should be reported. Some authors consider them to be diagnostic criteria for some forms of achalasia and for diffuse spasms (DES) (85,86). The CCH does not assign a precise meaning to them. They sometimes follow respiratory movements.
Conclusions
- Spontaneous activity in the form of simultaneous esophageal contractions is not seen in young healthy subjects and should therefore be considered as pathological. It indicates "esophageal irritability" and can be seen in esophageal motor disorder or GERD.
Should spontaneous activity and activity not related to protocol swallows be assessed?
Forty-five per cent of respondents thought assessment was required only when activity was relevant and unrelated to intubation; 25%, only if associated with symptoms; 15% considered that it should always be assessed, and another 15%, that it should not be assessed.
Current situation
The spontaneous activity in the form of simultaneous esophageal contractions (tertiary waves in classical terminology) is common in the elderly and is not observed in young healthy subjects; it should therefore be considered as pathological in this population group. It indicates "esophageal irritability" and can be seen in esophageal motor disorders or GERD.
Although they are not included in the CCH, in "conventional" manometry their presence is considered as a manometric diagnostic criterion for DES (87). Clearly abnormal contractions that are unrelated to programmed swallows are often recorded. They are not included in the CCH, but they may have clinical significance.
Conclusions
- The presence and possible causal mechanism of simultaneous contractions and of contractile activity recorded "off-protocol" should be described in the final report according to its characteristics, frequency, and likely clinical relevance.
Should secondary waves be assessed?
Eighty per cent of respondents felt that their presence should be reported but without influencing the assessment of other waves.
Current situation
The characteristics of secondary peristalsis are well known (88,89) and can be easily seen with HRM; however, they are not covered by the CCH. They are defined as peristaltic contractions that are not preceded by swallowing, that respond to the stimulation of mechanoreceptors and/or chemoreceptors of the esophageal wall and the aim of which is to "cleanse" the esophageal body content. They may appear as a consequence of a swallow with weak primary peristalsis that did not effectively clear the swallowed bolus, due to partial retention of swallowed material caused by distal flow obstruction (high IRP), or in response to an episode of GER. HRM can easily identify both situations.
Conclusions
- Although they are a physiological response to the presence of esophageal intraluminal content, if they are frequent during the study, their presence should be reported in the report along with their possible causal mechanism.
What parameters should be analyzed?
One hundred per cent of those attending believed that the IRP-4s should be analyzed, and 90% considered the DCI, the resting pressure of the EGJ and the integrity of the contractile front to be susceptible to analysis. Eighty per cent thought that the total length of the LES should be indicated, 75% focused on the pressure inversion point; 70%, on the intrabolus pressure and distal latency; 60%, on the contractile front velocity, and 45%, on the length of the LES abdominal portion.
Current situation
In the CCH version 3.0 (3) the classical parameters of contraction in the esophageal body (wave amplitude, velocity and duration) are combined into a single parameter called DCI, which defines the force or strength of the contraction. Weak contractions with values below 450 mmHg cm-1/s-1, or failed peristalsis (interrupted) below 100 mmHg cm-1/s-1 are considered as ineffective contractions. Peristaltic waves with DCI > 8,000 mmHg cm-1/s-1 are considered to be hyper-contractile, and a hyper-contractile esophagus is defined by the presence of at least 20% of contractions with DCI > 8,000 mmHg cm-1/s-1. The morphology, the type of contraction and the relationship between the contraction of the esophageal body and the EGJ resistance to flow are determined only with waves with DCI > 450 mmHg cm-1/s-1 using criteria based on distal latency and the isobaric contour > 20 mmHg.
Regarding the evaluation of the EGJ resistance to flow by determining the intrabolus pressure, pan-pressurization and compartmentalized pressurization of the UEG, its limits are not clear, nor is it clear whether to consider using values above 17 mmHg (67) or only with pressurization > 30 mmHg as measured by the isobaric contour (3).
Conclusions
- There is insufficient clarity on the clinical significance or how to grade patients presenting contractions with values between 5,000 and 8,000 mmHg cm-1/s-1, according to different criteria (95th percentile or never seen in normal subjects) but both with sufficient specific weight.
- It is difficult to assess these amendments as they were published only recently. Although these changes are generally considered as appropriate, their application to everyday clinical practice presents some difficulties. In general, a careful assessment of the new criteria is deemed as necessary once more experience has been gained on how to apply them.
How should the multiple swallow test be performed?
Sixty per cent of respondents felt it should be done with the patient seated and 25% opted for supine position; 45% felt that the patient should drink directly from the glass and for a 30% a "straw" should be used. In terms of volume, 45% felt that 100 cc should be given, and 25%, that 200 cc are required.
In order to evaluate the rapid swallow test, 40% felt that a series of small volumes of water should be given.
What is assessed in the multiple swallow test?
Seventy-five per cent of respondents considered that the object of assessment is whether inhibition occurs in the esophageal body and the LES in addition to retention in the esophagus; 80% considered the presence or absence of an effective contraction following the last swallow as the object of analysis; 65% thought the test focusses on the characteristics of this contraction; and 5% considered it assesses whether the test was completed.
Current situation
Both the rapid swallow test (RS) (4-6 swallows of 5 ml every 2-3 seconds) (90,91) and the stress test with multiple swallows (MS) (100-200 ml with swallows in quick succession without breaks) (40,41,94) are easy to perform and do not require a significant prolongation of the test, so they should be performed to complete the HRM study.
The RS test should be done with the patient recumbent, administering the bolus by syringe. In the MS test the patient should be sitting and drinking with a straw or directly from the cup. Drinking from the cup is more physiological but not always easier, because if more than three seconds elapse between swallows the test is no longer valid (94). The RS test is especially suitable for patients with hypomotility, as it allows the functional peristaltic reserve that has been linked with the appearance of dysphagia after fundoplication (91,95,96) to be assessed.
Regarding the stress test with MS, although a 200 ml volume can discriminate better than one of 100 ml, many patients with severe dysphagia do not tolerate it (94).
Unlike what occurs after the RS test, the absence of a final peristaltic wave after the stress test with MS does not appear to be relevant (it does not show up in 50% of normal controls) (40,41,94).
The MS stress test is especially suitable for patients with dysphagia (94,96). It is highly recommended when medical records are compatible with achalasia but with IRP below the lower limit (specific to the equipment used), in tracings with increased flow resistance and in patients with esophageal-gastric surgery (92). In some cases, studies with impedance can be useful, having been related to radiological contrast studies in patients with achalasia (93).
Conclusions
- The RS and MS tests are easy to perform and do not excessively prolong the examination.
- The RS test evaluates the functional peristaltic reserve of the esophagus, which may be important in patients with hypomotility-type motor disorders.
- The MS test is useful in the study of dysphagia. It is therefore recommended that it be performed as part of the HRM study.
What is assessed in the upper esophageal sphincter?
Ninety per cent of respondents felt that the objects of assessment are the resting and residual pressures, the length and the contractile activity with and without swallowing.
Current situation
The UES resting pressure varies throughout the study, and the value obtained at the end of the test will likely be more useful with regard to symptoms (29). Although several studies have demonstrated that HRM is useful in identifying the motor behavior of the different elements involved in the pharyngo-esophageal phase of swallowing (97) and the prospect of automatically analyzing this area seems ever closer (98), the current situation shows that:
1. In the UES, the lower fascicle of the lower pharyngeal constrictor and the first few cm of the circular layer of the cervical esophagus work alongside the cricopharyngeal muscle.
2. The CCH does not provide criteria or analytical tools for the UES, although this does not prevent functional impairments from being recognized in different pathologies that affect this complex region.
3. The UES motor behavior should not be considered as an isolated event as it is closely linked to reflex mechanisms triggered at the level of the pharynx, esophageal body and/or EGJ.
4. Assessment of the morphology of the pharyngo-esophageal junction at baseline (without swallowing), and of the behavior of the pharynx, UES and upper esophagus after swallowing, can provide information that may improve the diagnostic and therapeutic approach to various degenerative and/or neurological pathologies.
Conclusions
- HRM is no doubt a great advance in the study of the UES. Currently, no specific software is available for assessing the pharynx and UES; however, it should not be studied in isolation from the rest of the esophagus.
What normal values are used in HRM?
Seventy per cent of respondents use the CCH values; 25% utilize the values by each manufacturer; 15%, the values of the classical system; 10%, the locally validated values, and 5% thought that there were no well-defined values.
Current situation
The findings made in conventional manometry studies, later confirmed by HRM, have described variations of normal values according to technical, ethnic and demographic factors. Moreover, HRM has modified concepts, parameters and assessment methods with clear differences between different analysis programs (32,34).
What normal values are used in HRM with impedanciometry?
The survey could not be evaluated due to the low number of responses.
Combined high resolution manometry studies with impedanciometry (HRM -I) are relatively recent, and neither their methodology nor their analysis parameters are completely defined. The normal values of this technique are based on various studies made with healthy volunteers using liquid and viscous boluses. Swallows with incomplete clearing were considered as pathological in over 20% of liquid swallows and over 30% of swallows with viscous boluses (99). A 2,400 Ω cutoff point was established to distinguish between patients with dysphagia and healthy controls (100). New studies are needed to confirm these results.
Conclusions
- It is recommended that, as far as possible, normal values are available for each laboratory. Failing that, values should be applied from studies made with equipment and protocols similar to those being used.
How should the report be drafted? (More than one answer)
Seventy per cent of respondents said that the CCH diagnosis should be included, 65% recommended a clinical diagnosis, 60% also thought that treatment recommendations should be included, and 50% deemed a summary of manometry results as necessary.
Current situation
The report must include general information and manometric aspects of the LES and esophageal body motor behavior; there is no unanimous agreement on whether the LES should be included or not. General information includes: patient identification, date, equipment used, indication, tolerance to the test, topical anesthesia, etc. The description of motility includes: EGJ morphology, the resting and relaxation pressures of the LES, baseline pressure of the esophageal body and the characteristics of motor behavior after swallowing (timing, amplitude and duration of contractions) (9). In general terms, it is recommended that the HRM guidelines established by the Mayo Clinic for conventional esophageal manometry be followed (9).
Conclusions
- The CCH leaves out of its assessment certain data that have so far been considered as essential, such as the LES resting pressure.
- It uses new, less commonly known concepts and terminology in non-specialized areas. It is important to use "understandable" terms, to try to stick to new classifications and to refer to well-established concepts whenever necessary.
- The possible relation to organic disorders (secondary motor disorders) should be considered, making treatment management recommendations whenever possible.
In summary, HRM is under development as is clear from the succession of Chicago classifications. Some practical aspects are not sufficiently well defined, whereas in other areas the fact that certain parameters have been recently introduced means that there is very little accumulated experience. The aim of this meeting was to guide and harmonize as far as possible the criteria to be followed in situations in daily practice where current guidelines are poorly defined. We are aware that decisions by consensus have a "limited value" compared to scientific evidence obtained in well-designed, randomized, double blind studies, and for this reason the conclusions of this meeting do not intend to be dogmatic, and do not attempt to impose criteria.
References
1. Carlson DA, Ravi K, Kahrilas PJ, et al. Diagnosis of esophageal motility disorders: Esophageal pressure topography vs. conventional line tracing. Am J Gastroenterol 2015;110(7):967-77;quiz78. DOI: 10.1038/ajg.2015.159. [ Links ]
2. Ciriza-de-los-Ríos C, Canga-Rodríguez-Valcárcel F. High-resolution manometry and impedance-pH/manometry: Novel techniques for the advancement of knowledge on esophageal function and their clinical role. Rev Esp Enferm Dig 2009;101(12):861-9. DOI: 10.4321/S1130-01082009001200006. [ Links ]
3. Kahrilas PJ, Bredenoord AJ, Fox M, et al. The Chicago Classification of esophageal motility disorders, v3.0. Neurogastroenterol Motil2015;27(2):160-74. DOI: 10.1111/nmo.12477. [ Links ]
4. Wang YT, Yazaki E, Sifrim D. High-resolution manometry: Esophageal disorders not addressed by the "Chicago Classification". J Neurogastroenterol Motil2012;18(4):365-72. DOI: 10.5056/jnm.2012.18.4.365. [ Links ]
5. Castell JA, Castell DO. Manometría esofágica. En: Scarpignato C,Galmiche J, editores. Exploraciones funcionales en la enfermedad esofágica: EDIKA MED; 1994. p. 109-29. [ Links ]
6. Mansson I, Sandberg N. Oro-pharyngeal sensitivity and elicitation of swallowing in man. Acta Otolaryngol 1975;79:140-5. DOI: 10.3109/00016487509124666. [ Links ]
7. Carmona-Sánchez R, Valerio Ureña J, Valdovinos Díaz MA. The usefulness of lidocaine in gel in esophageal manometry. Rev Gastroenterol Mex 2001;66(3):137-40. [ Links ]
8. Carmona-Sánchez R, Esmer-Sánchez D, Tostado-Fernández FA. Comparison of two forms of nasal and pharyngeal topical anesthesia for performing esophageal manometry. Rev Gastroenterol Mex 2007;72(2):100-3. [ Links ]
9. Murray JA, Clouse RE, Conklin JL. Components of the standard oesophageal manometry. Neurogastroenterol Motil 2005;15:591-606. DOI: 10.1046/j.1365-2982.2003.00446.x. [ Links ]
10. Tutuian R. Adverse effects of drugs on the esophagus. Gastroenterology 2010;24:91-7. DOI: 10.1016/j.bpg.2010.02.005. [ Links ]
11. Stacher G, Schneider C, Steinringer H, et al. Effects of 3-days' intake of a sustained-release preparation of the nitric oxide donor, isosorbide dinitrate, on oesophageal motility. Aliment Pharmacol Ther 1997;11:967-71. DOI: 10.1046/j.1365-2036.1997.00241.x. [ Links ]
12. Ishikawa H, Iwakiri K, Sugiura T, et al. Effect of nifedipine administration (10 mg) on esophageal acid exposure time. J Gastroenterol 2000;35:43-6. DOI: 10.1007/s005350050008. [ Links ]
13. Yoshida K, Furuta K, Adachi K, et al. Effects of anti-hypertensive drugs on esophageal body contraction. World J Gastroenterol 2010;16:987-91. DOI: 10.3748/wjg.v16.i8.987. [ Links ]
14. Kim HS, Conklin JL, Park H. The effect of sildenafil on segmental oesophageal motility and gastro-oesophageal reflux. Aliment Pharmacol Ther 2006;24:1029-36. DOI: 10.1111/j.1365-2036.2006.03091.x. [ Links ]
15. Corley DA, Levin T, Habel LA, et al. Barrett's esophagus and medications that relax the lower esophageal sphincter. Am J Gastroenterol 2006;101:937-44. DOI: 10.1111/j.1572-0241.2006.00539.x. [ Links ]
16. Storr M, Allescher H. Esophageal pharmacology and treatment of primary motility disorders. Dis Esophagus 1999;12:241-57. DOI: 10.1046/j.1442-2050.1999.00059.x. [ Links ]
17. Scheerens C, Tack J, Rommel N. Buspirone, a new drug for the management of patients with ineffective esophageal motility? United European Gastroenterol J 2015;3(3):261-5. DOI: 10.1177/2050640615585688. [ Links ]
18. Blonski W, Vela M, Freeman J, et al. The effect of oral buspirone, pyridostigmine, and bethanechol on esophageal function evaluated with combined multichannel esophageal impedance-manometry in healthy volunteers. J Clin Gastroenterol 2009;43:253-60. DOI: 10.1097/MCG.0b013e318167b89d. [ Links ]
19. Kraichely RE, Arora A, Murray JA. Opiate-induced oesophageal dysmotility. Aliment Pharmacol Ther 2010;31:601-6. DOI: 10.1111/j.1365-2036.2009.04212.x. [ Links ]
20. Kessing BF, Smout AJ, Bennink RJ, et al. Prucalopride decreases esophageal acid exposure and accelerates gastric emptying in healthy subjects. Neurogastroenterol Motil 2014;26(8):1079-86. DOI: 10.1111/nmo.12359. [ Links ]
21. Di Stefano M, Papathanasopoulos A, Blondeau K, et al. Effect of buspirone, a 5-HT1A receptor agonist, on esophageal motility in healthy volunteers. Dis Esophagus 2012;25:470-6. DOI: 10.1111/j.1442-2050.2011.01275.x. [ Links ]
22. Broekaert D, Fischler B, Sifrim D, et al. Influence of citalopram, a selective serotonin reuptake inhibitor, on oesophageal hypersensitivity: A double-blind, placebo-controlled study. Aliment Pharmacol Ther 2006;23:365-70. DOI: 10.1111/j.1365-2036.2006.02772.x. [ Links ]
23. Jafari J, Yazaki E, Woodland P, et al. Effect of azithromycin on esophageal hypomotility (EH) and prediction of response by esophageal stimulations. Tests during high resolution manometry. Gastroenterology 2015;148(Suppl 1):S75. DOI: 10.1016/S0016-5085(15)30264-X. [ Links ]
24. Meyer GW, Castell D. Fisiología del esófago. Clínica Gastroenterológica Trastornos de la Motilidad: Ed. Esp. Salvat; 1984. p. 1-14. [ Links ]
25. Sifrim D, Janssens J, Vantrappen G. A wave of inhibition precedes primary peristaltic contractions in the human esophagus. Gastroenterology 1992;103:876-82. DOI: 10.1016/0016-5085(92)90020-Y. [ Links ]
26. Santander Vaquero C, Ruiz de León A. Manometría esofágica de alta resolución. En: Lacima G, Serra J, Mínguez M, Accarino A., editores. Tratado de neurogastroenterología y motilidad digestiva. Técnicas para el estudio de la función motora sensorial del tubo digestivo. Madrid: Panmericana; 2014. p. 56-66. [ Links ]
27. Soria de la Cruz MJ,Garrigues Gil V. Manometría esofágica convencional. En: Lacima G, Serra J, Mínguez M, Accarino A, editores. Tratado de neurogastroenterología y motilidad digestiva. Técnicas para el estudio de la función motora sensorial del tubo digestivo Madrid: Panamericana; 2014. p. 30-40. [ Links ]
28. Roman S, Kahrilas PJ, Boris L, et al. High-resolution manometry studies are frequently imperfect but usually still interpretable. Clin Gastroenterol Hepatol 2011;9(12):1050-5. DOI: 10.1016/j.cgh.2011.08.007. [ Links ]
29. Rezende DT, Herbella FA, Silva LC, et al. Upper esophageal sphincter resting pressure varies during esophageal manometry. Arq Bras Cir Dig 2014;27(3):182-3. DOI: 10.1590/S0102-67202014000300005. [ Links ]
30. Weihrauch TR. Factors influencing pressure recording. Esophageal, manometry methods and clinical practice: Urban&Schwarzenberg; 1981. p. 38-63. [ Links ]
31. Bredenoord AJ, Fox M, Kahrilas PJ, et al. Chicago classification criteria of esophageal motility disorders defined in high resolution esophageal pressure topography. Neurogastroenterol Motil 2012;24(Suppl 1):57-65. DOI: 10.1111/j.1365-2982.2011.01834.x. [ Links ]
32. Gyawali CP, Bredenoord AJ, Conklin JL, et al. Evaluation of esophageal motor function in clinical practice. Neurogastroenterol Motil 2013;25(2):99-133. DOI: 10.1111/nmo.12071. [ Links ]
33. Capovilla G, Salvador R, Savarino E, et al. Comparative assessment of tolerability, duration and costs between solid-state and water-perfused system for esophageal motility testing - Data from a prospective, randomized, double blind, crossover study. Gastroenterology 2014;146(Suppl 1):S-680-1. DOI: 10.1016/S0016-5085(14)62473-2. [ Links ]
34. Herregods TV, Roman S, Kahrilas PJ, et al. Normative values in esophageal high-resolution manometry. Neurogastroenterol Motil 2015;27(2):175-87. DOI: 10.1111/nmo.12500. [ Links ]
35. Bogte A, Bredenoord AJ, Oors J, et al. Normal values for esophageal high-resolution manometry. Neurogastroenterol Motil 2013;25(9):762-e579. DOI: 10.1111/nmo.12167. [ Links ]
36. Xiang X, Tu L, Zhang X, et al. Influence of the catheter diameter on the investigation of the esophageal motility through solid-state high-resolution manometry. Dis Esophagus 2013;26(7):661-7. DOI: 10.1111/dote.12029. [ Links ]
37. Bredenoord AJ, Hebbard G. Technical aspects of clinical high-resolution manometry studies. Neurogastroenterol Motil 2012;24(Suppl 1):5-10. DOI: 10.1111/j.1365-2982.2011.01830.x. [ Links ]
38. Weijenborg PW, Kessing BF, Smout AJ, et al. Normal values for solid-state esophageal high-resolution manometry in a European population - An overview of all current metrics. Neurogastroenterol Motil 2014;26(5):654-9. DOI: 10.1111/nmo.12314. [ Links ]
39. Ciriza-de-Los-Ríos C, Canga-Rodríguez-Valcárcel F, Lora-Pablos D, et al. How the body position can influence high-resolution manometry results in the study of esophageal dysphagia and gastroesophageal reflux disease. J Neurogastroenterol Motil 2015;21(3):370-9. DOI: 10.5056/jnm14110. [ Links ]
40. Sweis R, Anggiansah A, Wong T, et al. Assessment of esophageal dysfunction and symptoms during and after a standardized test meal: Development and clinical validation of a new methodology utilizing high-resolution manometry. Neurogastroenterol Motil 2014;26(2):215-28. DOI: 10.1111/nmo.12252. [ Links ]
41. Daum C, Sweis R, Kaufman E, et al. Failure to respond to physiologic challenge characterizes esophageal motility in erosive gastro-esophageal reflux disease. Neurogastroenterol Motil 2011;23(6):517-e200. DOI: 10.1111/j.1365-2982.2011.01669.x. [ Links ]
42. Ang D, Tucker E, Wright J, et al. High resolution manometry with multiple water swallows: A complementary role in the detection of esophageal pathology. Gastroenterology 2015;148(Suppl 1):S814-5. DOI: 10.1016/S0016-5085(15)32772-4. [ Links ]
43. Sweis R, Anggiansah A, Wong T, et al. Normative values and inter-observer agreement for liquid and solid bolus swallows in upright and supine positions as assessed by esophageal high-resolution manometry. Neurogastroenterol Motil 2011;23(6):509-e198. DOI: 10.1111/j.1365-2982.2011.01682.x. [ Links ]
44. Xiao Y, Read A, Nicodeme F, et al. The effect of a sitting vs supine posture on normative esophageal pressure topography metrics and Chicago Classification diagnosis of esophageal motility disorders. Neurogastroenterol Motil 2012;24(10):e509-16. DOI: 10.1111/j.1365-2982.2012.02001.x. [ Links ]
45. Pandolfino JE, Zhang QG, Ghosh SK, et al. Transient lower esophageal sphincter relaxations and reflux: Mechanistic analysis using concurrent fluoroscopy and high-resolution manometry. Gastroenterology 2006;131(6):1725-33. DOI: 10.1053/j.gastro.2006.09.009. [ Links ]
46. Mittal RK, Chiareli C, Liu J, et al. Characteristics of lower esophageal sphincter relaxation induced by pharyngeal stimulation with minute amounts of water. Gastroenterology 1996;111(2):378-84. DOI: 10.1053/gast.1996.v111.pm8690202. [ Links ]
47. Hershcovici T, Mashimo H, Fass R. The lower esophageal sphincter. Neurogastroenterol Motil 2011;23(9):819-30. DOI: 10.1111/j.1365-2982.2011.01738.x. [ Links ]
48. Kuribayashi S, Massey B, HafeezullahM, et al. Terminating motor events for TLESR are influenced by the presence and distribution of refluxate. Am J Physiol Gastrointest Liver Physiol 2009;297:G71-5. DOI: 10.1152/ajpgi.00017.2009. [ Links ]
49. Van Herwaarden MA, Katzka D, Smout AJ, et al. Effect of different recumbent positions on postprandial gastroesophageal reflux in normal subjects. Am J Gastroenterol 2000;95:2731-6. DOI: 10.1016/S0002-9270(00)01973-0. [ Links ]
50. Frankhuisen R, Van Herwaarden MA, Scheffer RC, et al. Increased intragastric pressure gradients are involved in the occurrence of acid reflux in gastroesophageal reflux disease. Scand J Gastroenterol 2009;44:545-50. DOI: 10.1080/00365520902718903. [ Links ]
51. Kwiatek MA, Pandolfino JE, Kahrilas PJ. 3D-high resolution manometry of the esophagogastric junction. Neurogastroenterol Motil 2011;23(11):e461-9. DOI: 10.1111/j.1365-2982.2011.01733.x. [ Links ]
52. Kahrilas PJ, Kim HC, Pandolfino JE. Approaches to the diagnosis and grading hiatal hernia. Best Pract Res Clin Gastroenterol 2008;22(4):601-16. DOI: 10.1016/j.bpg.2007.12.007. [ Links ]
53. Kahrilas PJ, Peters JH. Evaluation of the esophagogastric junction using high resolution manometry and esophageal pressure topography. Neurogastroenterol Motil 2012;24(Suppl 1):11-9. DOI: 10.1111/j.1365-2982.2011.01829.x. [ Links ]
54. Pandolfino JE, Ghosh SK, Zhang Q, et al. Quantifying EGJ morphology and relaxation with high-resolution manometry: A study of 75 asymptomatic volunteers. Am J Physiol Gastrointest Liver Physiol 2006;290(5):G1033-40. [ Links ]
55. Pandolfino JE, Kim H, Ghosh SK, et al. High-resolution manometry of the EGJ: an analysis of crural diaphragm function in GERD. Am J Gastroenterol. 2007;102(5):1056-63. DOI: 10.1111/j.1572-0241. 2007.01138.x. [ Links ]
56. Ciriza-de-los-Ríos C, Canga-Rodríguez-Valcárcel F, Castel-de-Lucas I, et al. How useful is esophageal high resolution manometry in diagnosing gastroesophageal junction disruption: Causes affecting this disruption and its relationship with manometric alterations and gastroesophageal reflux. Rev Esp Enferm Dig 2014;106(1):22-9. DOI: 10.4321/S1130-01082014000100004. [ Links ]
57. Bredenoord AJ, Weusten BL, Timmer R, et al. Intermittent spatial separation of diaphragm and lower esophageal sphincter favors acidic and weakly acidic reflux. Gastroenterology 2006;130(2):334-40. DOI: 10.1053/j.gastro.2005.10.053. [ Links ]
58. Hoshino M, Sundaram A, Mittal SK. Role of the lower esophageal sphincter on acid exposure revisited with high-resolution manometry. J Am Coll Surg 2011;213(6):743-50. DOI: 10.1016/j.jamcollsurg.2011.09.002. [ Links ]
59. Nicodeme F, Pipa-Muniz M, Khanna K, et al. Quantifying esophagogastric junction contractility with a novel HRM topographic metric, the EGJ-Contractile Integral: Normative values and preliminary evaluation in PPI non-responders. Neurogastroenterol Motil 2014;26(3):353-60. DOI: 10.1111/nmo.12267. [ Links ]
60. Pandolfino JE, El-Serag HB, Zhang Q, et al. Obesity: A challenge to esophagogastric junction integrity. Gastroenterology 2006;130(3):639-49. DOI: 10.1053/j.gastro.2005.12.016. [ Links ]
61. Ghosh SK, Pandolfino JE, Rice J, et al. Impaired deglutitive EGJ relaxation in clinical esophageal manometry: A quantitative analysis of 400 patients and 75 controls. Am J Physiol Gastrointest Liver Physiol 2007;293(4):G878-85. DOI: 10.1152/ajpgi.00252.2007. [ Links ]
62. Pandolfino JE, Kahrilas PJ. Presentation, diagnosis, and management of achalasia. Clin Gastroenterol Hepatol 2013;11(8):887-97. DOI: 10.1016/j.cgh.2013.01.032. [ Links ]
63. Ruiz de León San Juan A, Casabona Francés S, Mestanza Rivas Plata AL, et al. Presión integrada de relajación (IRP) en pacientes con acalasia. Estudio en sedestación. Rev Esp Enferm Dig 2013;105(Suppl 1):235-6. [ Links ]
64. Ortiz V, Poppele G, Alonso N, et al. Evaluation of esophagogastric junction relaxation by 4-second integrated relaxation pressure in achalasia using high resolution manometry with water-perfused catheters. Neurogastroenterol Motil 2014;26(11):1551-6. DOI: 10.1111/nmo.12415. [ Links ]
65. Xiao Y, Nicodeme F, Kahrilas PJ, et al. Optimizing the swallow protocol of clinical high-resolution esophageal manometry studies. Neurogastroenterol Motil 2012;24(10):e489-96. DOI: 10.1111/j.1365-2982.2012.01989.x. [ Links ]
66. Do Carmo GC, Jafari J, Sifrim D, et al. Normal esophageal pressure topography metrics for data derived from the Sandhill-Unisensor high-resolution manometry assembly in supine and sitting positions. Neurogastroenterol Motil 2015;27(2):285-92. DOI: 10.1111/nmo.12501. [ Links ]
67. Lin Z, Kahrilas PJ, Roman S, et al. Refining the criterion for an abnormal integrated relaxation pressure in esophageal pressure topography based on the pattern of esophageal contractility using a classification and regression tree model. Neurogastroenterol Motil 2012;24(8):356-63. DOI: 10.1111/j.1365-2982.2012.01952.x. [ Links ]
68. Jung HY, Puckett JL, Bhalla V, et al. Asynchrony between the circular and the longitudinal muscle contraction in patients with nutcracker esophagus. Am J Gastroenterol 2005;128(5):1179-86. DOI: 10.1053/j.gastro.2005.02.002. [ Links ]
69. Mittal RK, Holloway RH, Penagini R, et al. Transient lower esophageal sphincter relaxation. Gastroenterology 1995;109:601-10. DOI: 10.1016/0016-5085(95)90351-8. [ Links ]
70. Sifrim D, Tack J, Zhang X, et al. Continuous monitoring of esophageal shortening in man during swallowing, transient LES relaxations and intraesophageal acid perfusion. Gastroenterology 2002;122(Suppl 1):188. [ Links ]
71. Shi G, Pandolfino JE, Joehl RJ, et al. Distinct patterns of oesophageal shortening during primary peristalsis, secondary peristalsis and transient lower oesophageal sphincter relaxation. Neurogastroenterol Motil 2002;14:505-12. DOI: 10.1046/j.1365-2982.2002.00351.x. [ Links ]
72. Lee YY, Whiting J, Robertson EV, et al. Kinetics of transient hiatus hernia during transient lower esophageal sphincter relaxations and swallows in healthy subjects. Neurogastroenterol Motil 2012;24(11):990-e539. DOI: 10.1111/j.1365-2982.2012.01948.x. [ Links ]
73. Sifrim D, Holloway R. Transient lower esophageal sphincter relaxations: How many or how harmful? Am J Gastroenterol 2001;96:2529-32. DOI: 10.1111/j.1572-0241.2001.04095.x. [ Links ]
74. Hong SJ, Bhargava V, Jiang Y, et al. A unique esophageal motor pattern that involves longitudinal muscles is responsible for emptying in achalasia esophagus. Gastroenterology 2010;139(1):102-11. DOI: 10.1053/j.gastro.2010.03.058. [ Links ]
75. Jiang Y, Bhargava V, Kim YS, et al. Esophageal wall blood perfusion during contraction and transient lower esophageal sphincter relaxation in humans. Am J Physiol Gastrointest Liver Physiol 2012;303(5):G529-35. DOI: 10.1152/ajpgi.00200.2012. [ Links ]
76. Mittal RK. Esophageal function testing: Beyond manometry and impedance. Gastrointest Endosc Clin N Am 2014;24(4):667-85. DOI: 10.1016/j.giec.2014.06.006. [ Links ]
77. Park JH. Clinical significance of esophageal hypertensive peristaltic contractions on high-resolution manometry. J Neurogastroenterol Motil 2015;21(4):616-7. DOI: 10.5056/jnm15106. [ Links ]
78. Weihrauch TR. Manometric findings in different motor disorders. Esophageal Manometry Methods and Clinical Practice: Urban& Schwarzenberg; 1981. p. 109-22. [ Links ]
79. Hirano I, Tatum RP, Shi G, et al. Manometric heterogeneity in patients with idiopathic achalasia. Gastroenterology 2001;120:789-98. DOI: 10.1053/gast.2001.22539. [ Links ]
80. Clouse RE, Staiano A, Alrakawi A. Topographic analysis of esophageal double-peaked waves. Gastroenterology 2000;118:469-76. DOI: 10.1016/S0016-5085(00)70252-6. [ Links ]
81. Roman S, Tutuian R. Esophageal hypertensive peristaltic disorders. Neurogastroenterol Motil 2012;24(Suppl 1):32-9. DOI: 10.1111/ j.1365-2982.2011.01837.x. [ Links ]
82. Sampath NJ, Bhargava V, Mittal RK. Genesis of multipeaked waves of the esophagus: Repetitive contractions or motion artifact? Am J Physiol Gastrointest Liver Physiol 2010;298(6):G927-33. DOI: 10.1152/ajpgi.00044.2010. [ Links ]
83. Roman S, Pandolfino JE, Chen J, et al. Phenotypes and clinical context of hypercontractility in high-resolution esophageal pressure topography (EPT). Am J Gastroenterol 2012;107(1):37-45. DOI: 10.1038/ajg.2011.313. [ Links ]
84. Martín-Domínguez V, Pérez-Fernández MT, Marinero A, et al. Hypercontractile esophagus: Clinical context and motors findings in high resolution manometry. Rev Esp Enferm Dig 2015;107(5):274-9. [ Links ]
85. Richter JE. Diffuse esophageal spasm. En: Castell DO, Richter J, Dalton ChB, editors. Esophageal motility testing: Elsevier Science Publishing; 1987. p. 118-29. [ Links ]
86. Fox MR, Bredenoord AJ. Oesophageal high-resolution manometry: Moving from research into clinical practice. Gut 2008;57(3):405-23. DOI: 10.1136/gut.2007.127993. [ Links ]
87. Stendal C. Practical guide to gastrointestinal function testing. Swallowing disorders: Alckwell Science Ltd. Medtronic Gastrointestinal; 1997. p. 27-45. [ Links ]
88. Chen C, Liu LT, Yi CH. Control of esophageal distension-induced secondary peristalsis by the GABAB agonist baclofen in humans. Neurogastroenterol Motil 2011;23:612-e250. DOI: 10.1111/j.1365-2982.2011.01716.x. [ Links ]
89. Ruiz de León, Farré Martí R. Función motora esofágica. En: Lacima G,Serra J, Mínguez M, Accarino A, editores. Tratado de neurogastroenterología y motilidad digestiva. Neurogastroenterología básica para clínicos. Madrid: Panamericana 2014. p. 110-20. [ Links ]
90. Fornari F, Bravi I, Penagini R, et al. Multiple rapid swallowing: A complementary test during standard oesophageal manometry. Neurogastroenterol Motil 2009;21:718-e41. DOI: 10.1111/j.1365-2982.2009.01273.x. [ Links ]
91. Shaker A, Stoikes N, Drapekin J, et al. Multiple rapid swallow responses during esophageal high-resolution manometry reflect esophageal body peristaltic reserve. Am J Gastroenterol 2013;108(11):1706-12. DOI: 10.1038/ajg.2013.289. [ Links ]
92. Wang YT, Tai LF, Yazaki E, et al. Investigation of dysphagia after antireflux surgery by high resolution manometry: Impact of multiple water swallows and a solid test meal on diagnosis, management and clinical outcome. Clin Gastroenterol Hepatol 2015;13:1575-83. DOI: 10.1016/j.cgh.2015.04.181. [ Links ]
93. Cho YK, Lipowska AM, Nicodeme F, et al. Assessing bolus retention in achalasia using high-resolution manometry with impedance: A comparator study with timed barium esophagram. Am J Gastroenterol 2014;109(6):829-35. DOI: 10.1038/ajg.2014.61. [ Links ]
94. Marin I, Serra J. Patterns of esophageal pressure responses to a rapid drink challenge test in patients with esophageal motility disorders. Neurogastroenterol Motil 2015. DOI: 10.1111/nmo.12749. [ Links ]
95. Stoikes N, Drapekin J, Kushnir V, et al. The value of multiple rapid swallows during preoperative esophageal manometry before laparoscopic antireflux surgery. Surg Endosc 2012;26(12):3401-7. DOI: 10.1007/s00464-012-2350-0. [ Links ]
96. Elvevi A, Mauro A, Pugliese D, et al. Usefulness of low- and high-volume multiple rapid swallowing during high-resolution manometry. Dig Liver Dis 2015;47(2):103-7. DOI: 10.1016/j.dld.2014. 10.007. [ Links ]
97. Takasaki K, Umeki H, Enatsu K, et al. Investigation of pharyngeal swallowing function using high-resolution manometry. Laryngoscope 2008;118(10):1729-32. DOI: 10.1097/MLG.0b013e31817dfd02. [ Links ]
98. Mielens JD, Hoffman M, Ciucci MR, et al. Automated analysis of pharyngeal pressure data obtained with high-resolution manometry. Dysphagia 2011;26(1):3-12. DOI: 10.1007/s00455-010-9320-2. [ Links ]
99. Tutuian R. Evaluating esophageal bolus transit by impedance monitoring. Gastrointest Endosc Clin N Am 2014;24(4):595-605. DOI: 10.1016/j.giec.2014.06.009. [ Links ]
100. Rommel N, Van Oudenhove L, Tack J, et al. Automated impedance manometry analysis as a method to assess esophageal function. Neurogastroenterol Motil 2014;26(5):636-45. DOI: 10.1111/nmo.12308. [ Links ]
![]() Correspondence:
Correspondence:
Constanza Ciriza-de-los-Ríos.
Department of Digestive Diseases.
Hospital Universitario 12 de Octubre.
Av. de Córdoba, s/n.
28041 Madrid, Spain
e-mail: constanzacarpa@gmail.com
Received: 02-06-2016
Accepted: 01-10-2016
