










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 n.3 Madrid Mar. 2017
PICTURES IN DIGESTIVE PATHOLOGY
Portal hydatid with secondary cavernomatosis
Hidatidosis portal con cavernomatosis secundaria
Ma Belén Rodríguez-Sanz, Ma del Mar Roldán-Cuena, Carlos Alberto Blanco-Álvarez and Raúl Sánchez-Jiménez
Department of General Surgery and Digestive Diseases. Complejo Asistencial de Ávila. Ávila, Spain
Case report
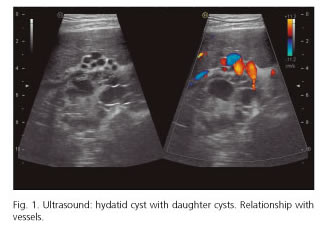
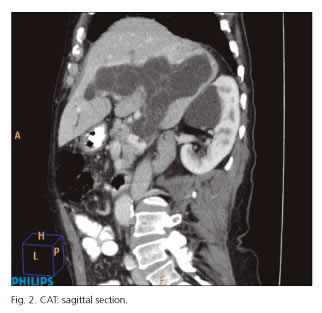
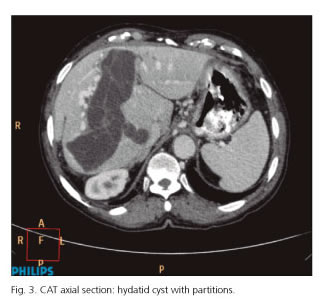
We report the case of an 81-year-old man treated for a hydatid cyst in segments VII-VIII six years before. The patient presented at the clinic due to discomfort in the right hypochondrium over a two-month period. Hydatid serology showed a titer of 1/800. An ultrasound was requested, which showed a cystic lesion with multiple daughter cysts of an elongated morphology and a size of 11 x 5.5 x 8.8 cm in the left, right and common portal vein in relation to portal hydatidosis (Fig. 1). The computed tomography (CT) scan revealed a cystic elongated, polylobulated and branched lesion of more than 14 cm of longitudinal diameter and 4 cm of transverse diameter occupying the interior of the right, left and main portal vein. As well as portal cavernomatosis with collateral circulation and esophageal varices (Figs. 2 and 3). The patient received medical treatment and is currently asymptomatic.
Discussion
The complication rate of hydatid cysts in the portal vein with cavernomatosis is very rare. There are few cases reported in the literature (1), the first one being described in 1998 (2).
Portal cavernomatosis is a dilatation of the paracholedochal and pericholedochal veins and it is generally secondary to portal vein thrombosis (3). It is an uncommon disease.
Portal involvement is caused by several mechanisms:
- Extrinsic compression.
- Invasion of vessels which looks like a thrombosis due to an inflammatory reaction in the vessel wall caused by external compression of the cyst, which facilitates the creation of a cyst-portal fistula thus allowing passage of daughter cysts to the vascular lumen.
- Cyst rupture, which occurs in 50-90% of cases.
The clinical manifestation is usually abdominal pain in the right hypochodrium with or without nausea and vomiting. The diagnosis is based on the detection of specific serum antibodies. Plain standard X-ray is used in imaging tests to detect calcified cysts, which occur in 20-30% of the cases.
Abdominal ultrasound is the most widely used technique since it is easy, inexpensive and has a sensitivity of 90-95%. In 1981, Gharbi et al. published an ultrasonographic classification based on structure and morphology. In 2003, the World Health Organization proposed a new classification, the World Health Organization Informal Working Group classification (WHO/IWG), based on the natural evolution of lesions.
The treatment of choice for portal hydatid disease is surgery, with the removal of the cyst. In recent years, due to the advances in liver surgery, hepatectomies are being performed with a low morbidity and mortality rate (4), including laparoscopic surgery. The authors have added praziquantel to the treatment schedule (5).
References
1. González E, Gil Grande L, Del Arbol L, et al. Presinusoidal portal hipertensión secondary to portal invasive echinococosis. J Clin Gastroenterol 2002;34:103-4. [ Links ]
2. Gil-Egea MJ, Alameda F, Girvent M, et al. Hydatid cyst in the hepatic hileum causing a cavernous transformation in the portal vein. Gastroenterol Hepatol 1998;21:227-9. [ Links ]
3. Pedrosa I, Saiz A, Aráosla J. Hydatid disease: Radiologic and pathologic features and complications. Radiographics 2000;20:795-817. DOI: 10.1148/radiographics.20.3.g00ma06795. [ Links ]
4. Priego P, Nuño J, López Hervás P, et al. Hidatidosis hepática. Cirugía radical vs. no radical: 22 años de experiencia. Rev Esp Enferm Dig 2008;100(2):82-5. DOI: 10.4321/S1130-01082008000200004. [ Links ]
5. Ramia JM, De la Plaza R, Casares M, et al. Profile of patients with hepatic hydatid disease not treated surgically. Rev Esp Enferm Dig 2011;103(9):448-52. DOI: 10.4321/S1130-01082011000900002. [ Links ]
