










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 no.3 Madrid mar. 2017
PICTURES IN DIGESTIVE PATHOLOGY
Long-standing indeterminate biliary stricture with iterative negative tissue sampling revealed as cholangiocarcinoma under SpyGlassTM cholangioscopy
Andrés Figueroa-Marrero, Carlos M. Chavarría-Herbozo, Carlos de-la-Serna-Higuera and Manuel Pérez-Miranda
Department of Gastroenterology. Hospital Universitario Río Hortega. Valladolid, Spain
Introduction
Bile duct brush cytology, intraductal biopsy and endoscopy ultrasound-guided fine needle aspiration (EUS-FN) are all used to characterize biliary strictures, with suboptimal sensitivity. Surgical resection without a confirmed malignancy is undesirable. Cholangioscopy with targeted biopsies appears to increase the diagnostic yield in indeterminate biliary strictures (1,2), but it is still considered as optional.
Case report
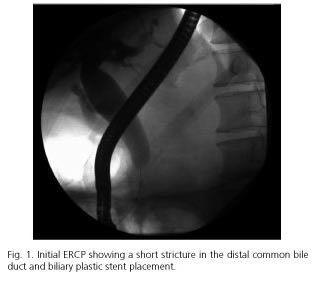
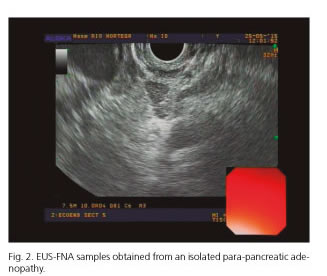
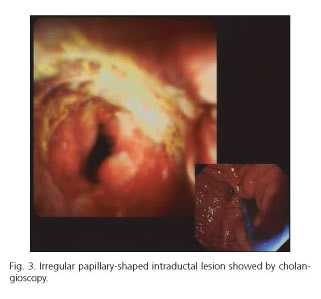
A 59-year-old man was admitted with acute cholangitis. Endoscopic retrograde cholangio-pancreatography (ERCP) revealed a short distal common bile duct stricture. Cytology brushings were obtained, and a biliary 10 F plastic stent was placed (Fig. 1). Over the next six months, four ERCPs were performed due to acute cholangitis episodes caused by stent dysfunction, with repeatedly negative brush cytology. No nodules or masses were seen on spiral computed tomography (CT) or EUS. EUS-FNA samples were obtained from a peripancreatic lymph-node retrieving normal lymphoid cells (Fig. 2). Surgical resection was considered two months after presentation, but eventually rejected in favor of temporary metal fully covered stent therapy. After a three-month period, the metal stent was removed and SpyGlassTM cholangioscopy was performed, revealing an irregular papillary-shaped intraductal lesion with a strong suspicion of malignancy (Fig. 3). Cholangioscopy guided biopsies were obtained. Histology revealed an infiltrative papillary adenocarcinoma. The patient underwent an uneventful Whipple procedure. Histological assessment of the resection specimen showed a T2 cholangiocarcinoma.
Discussion
Our case is remarkable because of the negative, repeated efforts at tissue diagnosis which was overcome by cholangioscopy and the lack of tumor spread despite a final diagnosis and treatment eight months after the first presentation. Early use of cholangioscopy may allow the confirmation of malignant indeterminate biliary strictures, thus avoiding the uncertainty of clinical follow-up or surgical resection in the absence of a confirmed malignancy (3).
References
1. Ramchandani M, Reddy DN, Gupta R, et al. Role of single-operator peroral cholangioscopy in the diagnosis of indeterminate biliary lesions: A single-center, prospective study. Gastrointest Endosc 2011;74:511-9. DOI: 10.1016/j.gie.2011.04.034. [ Links ]
2. Manta R, Frazzoni M, Conigliaro R, et al. SpyGlass single-operator peroral cholangioscopy in the evaluation of indeterminate biliary lesions: A single-center, prospective, cohort study. Surg Endosc 2013;27:1569-72. DOI: 10.1007/s00464-012-2628-2. [ Links ]
3. Woo YS, Lee JK, Oh SH, et al. Role of SpyGlass peroral cholangioscopy in the evaluation of indeterminate biliary lesions. Dig Dis Sci 2014;59:2565-70. DOI: 10.1007/s10620-014-3171-x. [ Links ]
