










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 n.3 Madrid Mar. 2017
https://dx.doi.org/10.17235/reed.2017.4291/2016
CASE REPORT
Central pancreatectomy for the treatment of a benign pancreatic lesion. Case report and literature review
Pancreatectomía central en el tratamiento de lesión pancreática benigna. Presentación de un caso y revisión de la literatura
Iván Domínguez-Sánchez, Ramón Gómez-Sanz, María Victoria Vieiro-Medina, Mónica Galán-Martín and Felipe de-la-Cruz-Vigo
Department of General and Digestive Surgery. Hospital Universitario 12 de Octubre. Madrid, Spain
ABSTRACT
We present the case of a 45 year old female patient with an incidental diagnosis of a cystic pancreatic lesion corresponding to a serous cystadenoma of 14 mm. During a 5-year follow-up (CT and MRT) the lesion tripled in size and a surgical intervention was decided upon. The lesion was thought to have a benign pathology and, in an attempt to preserve the spleen and a major portion of pancreatic tissue, a central pancreatectomy with a diversion of the remaining distal pancreas was carried out. The authors reviewed national and international publications.
Key words: Central pancreatectomy. Mesopancreatectomy. Benign pancreatic lesion.
RESUMEN
Presentamos el caso de una mujer de 45 años diagnosticada incidentalmente de lesión quística pancreática compatible con cistoadenoma seroso de 14 mm. Tras cinco años de seguimiento (TAC y RM) la lesión triplicó su tamaño y se indicó la intervención. Teniendo en cuenta la probable benignidad de la lesión, y en un intento de preservar tanto el bazo como la mayor cantidad posible de parénquima pancreático, se realizó una pancreatectomía central con derivación del remanente distal. Se revisa la literatura nacional e internacional publicada.
Palabras clave: Pancreatectomía central. Mesopancreatectomía. Lesión benigna pancreática.
Introduction
Central pancreatectomy (CP) is a pancreatic parenchyma-sparing technique, which can be used as a good alternative to major pancreatic resections such as distal pancreatectomy (DP). In the published studies CP was performed for benign lesions (neuroendocrine tumors, cystadenomas, small-size intraparenchymal tumors untreatable by enucleation, etc.) and for low-grade malignant lesions (mucinous cystic neoplasms, intraductal papillary mucinous neoplasms [IPMNs], solid pseudopapillary neoplasms, etc.) located in the neck and proximal body of the pancreas.
CP diminishes the morbidity related with major pancreatic resections with a lower incidence of pancreatic insufficiency, both of the endocrine and exocrine functions; it also decreases the risk of post-splenectomy infection.
Although there are multiple international studies in the literature, after review of published Spanish studies, we only found a few studies published by hospital centers in Navarra (1-6).
Case report
A 45-year-old woman with a long-term history of rheumatoid arthritis was diagnosed with a 14-mm unilocular cystic lesion in the pancreatic body during ultrasonography in 2009. The patient was under the care of the Gastroenterology Department and in 2010 they requested MRT and upper endoscopic ultrasound with a fine needle aspiration biopsy which revealed serous material without atypias. The study of serum tumor markers showed normal levels of CEA and trypsin with a CA 19.9 of 34.77 U/ml (normal range 0-27 U/ml).
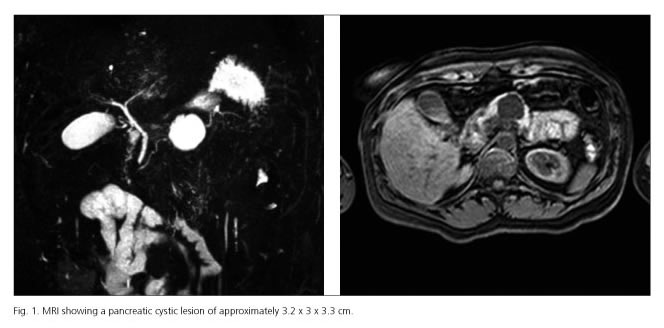
Finally, the patient was diagnosed with a cystic lesion in the pancreatic body compatible with a serous cystadenoma. Follow-up involved ultrasonography and due to the progressive growth, CT and MRI were performed in 2014, showing a cystic lesion of approximately 3.2 x 3 x 3.3 cm, which had tripled in size in comparison to the previous MR study.
Although the patient was asymptomatic, when considering the tumor growth during follow-up and the wishes of the patient, a surgical resection of the lesion by CP was decided upon.
After right transverse laparotomy the superior and inferior margins of the body and tail of the pancreas were dissected, allowing the identification of a 3-4 cm size cystic lesion in the pancreatic isthmus, which seemed to be benign. Pancreatic section was made proximal to the portal vein followed by interrupted polypropylene suture of the pancreatic stump. Then a dissection and resection of the central part of the pancreas containing the lesion was performed, preserving the splenic artery and vein. The distal pancreas was diverted performing Roux-en-Y pancreaticojejunostomy with a jejunal limb of 60 cm. Reinforcement of the anastomosis was done with a liquid fibrin sealant and an aspiration drainage was placed in the proximity of the anastomosis.
There were no postoperative complications observed and the patient was discharged on the ninth day after surgery with normal blood glucose levels. The pathology study of the lesion confirmed the diagnosis of a serous cystadenoma.
After a 16-month follow-up, the patient remains asymptomatic, with no exocrine or endocrine pancreatic insufficiency, and has not been hospitalized as a consequence of the surgery.
Discussion
Frequent use of imaging studies (ultrasonography and CT) as diagnostic techniques has led to an increase in the incidental discovery of pancreatic lesions, which are generally benign, asymptomatic and present a new challenge with regard to management and follow-up.
When it comes to dealing with benign lesions of the isthmus and proximal body of the pancreas which cannot be treated with enucleation (large lesions or lesions close to the duct of Wirsung), the usual techniques performed are a distal pancreatectomy (DP) or central pancreatectomy (CP)(3-5). The classic approach with DP involves the complete resection of the body and tail of the pancreas; however, CP allows the preservation of the distal pancreas, without the need of a splenectomy. CP requires a central localization of the lesion, with the preservation of the pancreatic stump.
Central pancreatectomy, which was carried out for the first time by Dagradi and Serio, consists of the resection of the pancreatic isthmus followed by diversion of the stump by pancreatojejunostomy or by pacreatogastrostomy (1,2).
Different studies comparing both procedures (CP versus DP) have shown a higher incidence of short-term morbidity associated with CP. Among the complications, of note is the risk of pancreatic fistula of approximately 30-40%, which is related to the presence of two surgical borders in the case of CP (1,3,4). As these benign lesions are in normal pancreatic tissue, they tend to have a soft consistency and the duct of Wirsung tends to have a small diameter, which results in a higher risk of anastomotic leak. With regard to the fistulization risk related to the type of the pancreatic anastomosis, the cumulative incidence of fistula seems to be higher in the pancreatojejunostomy than in the pacreatogastrostomy; nevertheless, the first procedure has a lower risk of exocrine insufficiency. The reintervention risk for fistula is low (about 4%), meanwhile a conservative management gives good results (1,2,7,8).
Central pancreatectomy seems to reduce the intraoperative blood loss, but it is associated with an increase in the surgery time which is related to the meticulousness required in this type of procedure (1,3,9).
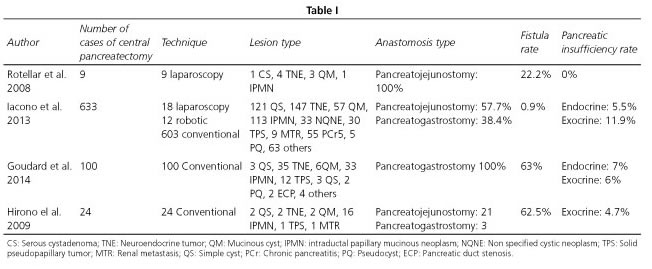
When evaluating long-term results, it is worth mentioning the benefit of CP in preserving the pancreatic function (6-7). According to the meta-analysis performed by Iacono et al. in 2013, the risk of endocrine insufficiency in CP was 5.5% versus 23.6% in the case of DP. With regard to exocrine function, the percentage would be 11.9% versus 19.1% (1,3). On a national level, the study performed by Herrera-Cabezón et al. should be mentioned, which reviews 480 pancreatic resections, among them ten CP. The indications for CP were three IPMNs, four cystadenomas and three neuroendocrine tumors. The fistula rate was 70-80%, which were managed in a conservative manner (8). Valentí-Azcárate et al. in 2005 described three cases of CP, two cases of mucinous cystadenoma and one of a serous cystadenoma (5).
With regard to the approach, conventional surgery is described in the majority of the studies, with the adaptation of the technique with laparoscopic and robot-assisted surgery (2,5,10). A series of nine laparoscopic central pancreatectomies, which had favorable results, published by Rotellar et al. in 2008 are worth mentioning (10).
Conclusion
Central pancreatectomy as a parenchyma preserving technique can be an excellent surgical option for patients with benign lesions or with low-grade malignant lesions (cystic or non-cystic) with a central location and with normal parenchyma. The high level of complexity of this technique should be noted, as well as the probable higher rate of pancreatic fistula during the postoperative period (1,3,5).
References
1. Iacono C, Verlato G, Ruzzenente A, et al. Systematic review of central pancreatectomy and meta-analysis of central versus distal pancreatectomy. Wyley Online Library 2013. DOI: 10.1002/bjs.9136. [ Links ]
2. Iacono C, Ruzzenente A, Bortolasi L, et al. Central pancreatectomy: The Dagradi Serio Iacono operation. Evolution of a surgical technique from the pioneers to the robotic approach. World J Gastroenterol 2014;20(42):15674-81. DOI: 10.3748/wjg.v20.i42.15674. [ Links ]
3. Goudar Y, Gujoux S, Dokmak S, et al. Reappraisal of central pancreatectomy: A 12-year single-center experience. JAMA Surg 2014:149(4):356-63. DOI: 10.1001/jamasurg.2013.4146. [ Links ]
4. Beger H. G, Siech M, Poch B, et al. Limited surgery for benign tumours of the pancreas: A systematic review. World J Surg 2015;39:1557-66. DOI: 10.1007/s00268-015-2976-x. [ Links ]
5. Valentí-Azcárate V, Pardo-Sánchez F, Rotellar-Sastre F, et al. Pancreatectomía central en tumores benignos del cuello del páncreas. Cir Esp 2005;78(6):388-90 DOI: 10.1016/S0009-739X(05)70961-1. [ Links ]
6. Cienfuegos J.A, Rotellar F, Martí Cruchaga P, et al. Neoplasia papilar mucinosa intraductal del páncreas: Resultados clínico-patológicos. Rev Esp Enferm Dig 2010;102(5):314-20. DOI: 1130-0108/2010/102/5/314-320. [ Links ]
7. Hirono S, Tani M, Kawai M, et al. A central pancreatectomy for benign or low-grade malignant neoplasm. J Gastrointes Surg 2009;13:1659-65. DOI: 10.1007/s11605-009-0934-0934. [ Links ]
8. Herrera-Cabezón F, Pablo Sánchez-Acedo P, Cruz Zazpe-Ripa C, et al. Estándares de calidad en 480 resecciones pancreáticas: estudio prospectivo observacional. Rev Esp Enferm Dig 2015;107(3):143-51. DOI: 1130-0108/2015/107/3/143-151. [ Links ]
9. Del Chiaro M. Are there really indications for central pancreatectomy? JAMA Surg 2014;149(4):364. DOI: 10.1001/jamasurg.2013.4166. [ Links ]
10. Rotellar F, Pardo F, Montiel C, et al. Totally laparoscopic Roux-en-Y ducto-to-mucosa pancreaticojejunostomy after middle pancreatectomy. Ann Surg 2008;247:938-44. DOI:10.1097/SLA. 0b013e3181724e4a. [ Links ]
![]() Correspondence:
Correspondence:
Iván Domínguez Sánchez.
Department of General and Digestive Surgery.
Hospital Universitario 12 de Octubre.
Av. de Córdoba, s/n.
28041 Madrid, Spain
e-mail: drdomsan86@gmail.com
Received: 12-03-2016
Accepted: 11-04-2016
