










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 no.4 Madrid abr. 2017
PICTURES IN DIGESTIVE PATHOLOGY
An unusual enterolith ileus
Ismael Mora-Guzmán, José Luis Muñoz de Nova and Ana Rodríguez Sánchez
Department of General and Digestive Surgery. Hospital Universitario de La Princesa. Madrid, Spain
Case report
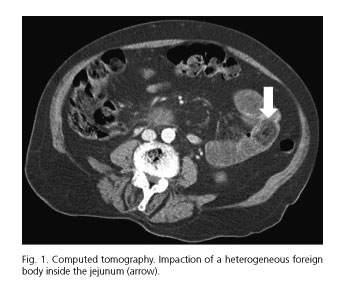
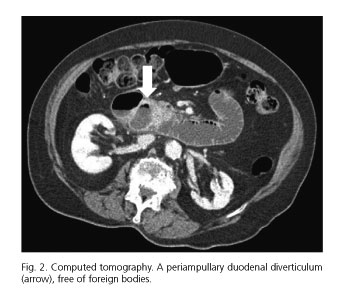
An 86-year-old woman with cognitive impairment and without a previous history of surgery presented with abdominal pain, vomiting, and absence of fecal deposition in the previous three days. Physical examination showed a painful, distended and tympanic abdomen. Laboratory tests revealed white cell count of 13.9 x 109/L, and plain abdominal X-ray showed severe gastric dilation. Computed tomography (CT) revealed dilation of the duodenum and a heterogeneous opacity inside the jejunum (Fig. 1), which suggested an enterolith. A large duodenal diverticulum was also found located periampullary (Fig. 2). A conservative treatment was performed with a nasogastric tube, draining 800 ml. After 24 hours, the patient needed an emergency laparotomy, which confirmed an intraluminal impaction, and enterotomy was performed. Histologic examination identified a solid sample measuring 4.5 cm, confirming a phytobezoar.
Discussion
Enterolith ileus (EI) is caused by migration of an unknown body and its secondary impaction in a distant part of the bowel. EI secondary to duodenal diverticula is an exceptional entity. Less than ten cases have been described so far (1,2).
It is not possible to differentiate clinically EI from gallstone ileus. Therefore, to make a correct diagnosis, both the absence of gallstones in the biliary tree and the presence of a small bowel diverticula need to be established (2).
Conservative treatment is unsuccessful in most cases, requiring a subsequent emergency surgical exploration to verify a normal biliary tree and to locate the site of impaction and diverticulosis. When a manual fragmentation of the piece is not possible an enterotomy must be performed (1-3).
References
1. Monchal T, Hornez E, Bourgouin S, et al. Enterolith ileus due to jejunal diverticulosis. Am J Surg 2010;199:e45-7. DOI: 10.1016/j.amjsurg.2009.05.042. [ Links ]
2. Medsinge A, Remer EM, Winans CG. Duodenal diverticulitis followed by enterolith-associated small bowel obstruction. Emerg Radiol 2012;19:261-4. DOI: 10.1007/s10140-012-1019-2. [ Links ]
3. Franzen D, Gürtler T, Metzger U. Solitary duodenal diverticulum with enterolith as a rare cause of acute abdomen. Swiss Surg 2002;8:277-9. DOI: 10.1024/1023-9332.8.6.277. [ Links ]
