










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 n.4 Madrid Apr. 2017
https://dx.doi.org/10.17235/reed.2016.4209/2016
CASE REPORT
Colonic obstruction secondary to sigmoid fecaloma endoscopically resolved with Coca-Cola®
Obstrucción colónica secundaria a fecaloma de sigma resuelta endoscópicamente con Coca-Cola®
Guillermo Ontanilla-Clavijo, Rafael León-Montañés, Yolanda Sánchez-Torrijos, Teófilo López-Ruiz and Juan Manuel Bozada-García
Department of Clinical Management of Digestive Diseases. Hospital Universitario Virgen del Rocío. Sevilla, Spain
ABSTRACT
Background: Colonic obstruction is a relatively common condition in emergency care, with a mortality rate of up to 20%. In 90% of cases it results from colonic or rectal adenocarcinoma, volvulus, or stenosis secondary to diverticular disease. When fecal impaction is the underlying cause, the condition is usually managed conservatively, but may on occasion become complicated and even require surgical intervention. Based on the proven efficacy of Coca-Cola® to dissolve gastric phytobezoars, we report a case of colonic obstruction secondary to sigmoid fecaloma.
Case report: A 58 years old woman arrived at the Emergency Room (ER) with persistent constipation for the last six days. An abdominal CT scan showed a large fecal mass at the sigmoid colon with retrograde dilated colonic loops. Cleansing enemas and oral lactulose were administered, which failed to resolve the clinical presentation, so we then proceeded to inject Coca-Cola® within the fecaloma using a sclerosing needle, and then washed the fecaloma surface also with Coca-Cola®. After a few minutes we started to fragment the fecalith, the consistency of which had been notably decreased.
Discussion: The use of Coca-Cola® for gastric washes in the management of phytobezoars is well established. Since fecaliths are partly composed of these same substances than phytobezoars, the use of Coca-Cola® might well be warranted against them as in our patient, without surgery. Our case report is the second one published in the literature, in which Coca-Cola® helped solve colonic obstruction secondary to fecaloma.
Key words: Obstruction. Colon. Fecaloma. Coca-Cola®. Endoscopy.
RESUMEN
Introducción: la obstrucción colónica es una patología relativamente frecuente en el área de urgencias, con una mortalidad de hasta el 20%. En el 90% de los casos se debe a adenocarcinoma de colon o recto, vólvulo o estenosis secundaria a enfermedad diverticular. Respecto a la impactación de material fecal como causa de la misma es una entidad que suele manejarse forma conservadora, aunque en ocasiones puede complicarse y precisar incluso de intervención quirúrgica para su resolución. Basándonos en la efectividad demostrada de la Coca-Cola® para disolver fitobezoars gástricos planteamos su uso en un caso de obstrucción colónica secundaria a fecaloma de sigma.
Caso clínico: se trata de una mujer de 58 años que acude a urgencias por cuadro de estreñimiento pertinaz de 6 días de evolución. En las pruebas radiológicas realizadas se demostró la presencia gran masa de material fecal impactada en colon sigmoides que condicionaba dilatación retrógrada de asas colónicas. Tras el fracaso de las medidas conservadoras con enemas de limpieza y lactulosa oral, se decidió desimpactar el fecaloma mediante colonoscopia valiéndonos de Coca-Cola®, que aplicamos con irrigaciones e inyección local. Esto disminuyó su consistencia y permitió la fragmentación con asa del fecaloma.
Discusión: la Coca-Cola® ya se emplea para disolver fitobezoars gástricos. La composición similar de los fecalomas hace suponer que esta sea también efectiva como así fue en el caso de nuestra paciente, permitiendo no tener que intervenir a la paciente. Nuestro caso es el segundo publicado en el que la Coca-Cola® ayudó a la resolución de una obstrucción colónica secundaria a fecaloma.
Palabras clave: Obstrucción. Colon. Fecaloma. Coca-Cola®. Endoscopia.
Introduction
Colonic obstruction is a relatively common condition in emergency care, with a mortality rate of up to 20%. In 90% of cases it results from colonic or rectal adenocarcinoma, volvulus, or stenosis secondary to diverticular disease. When fecal impaction is the underlying cause, the condition is usually managed conservatively, but may on occasion become complicated and even require surgical intervention. Few data are available regarding frequency, which partly results from the fact it had no code in the USA before 2010, which prevented it being recorded in emergency care databases. From an analysis of the National Emergency Department Sample (NEDS) data, it is estimated that 42,481 emergency visits (EVs) occurred in 2011 which resulted in a diagnosis with fecal impaction, with a ratio of 32 visits/100,000 EVs. This diagnosis was most common for ageing patients (> 85 years; 176.8/100,000 EVs, with a mean age of 63.6 years (63.1-64.1, 95% CI), with women slightly predominating (34.2 vs 30.2/100,000 EVs; RR 1.13; 95% CI, 1.11-1.15). The mean cost per related EV was USD 3,060.47, for an overall cost of USD 130 million in 2011. The clinical significance of the condition and its potentially related complications, together with its non-negligible frequency and resulting financial cost, make it necessary to explore novel conservative management techniques. Based on the proven efficacy of Coca-Cola® to dissolve gastric phytobezoars, we report a case of colonic obstruction secondary to sigmoid fecaloma that was resolved by endoscopic irrigation with Coca-Cola® followed by fragmentation.
Case report
A 58-year-old woman with a history of high blood pressure and dyslipidemia, who occasionally took clebopride/simethicone prescribed by her Primary Care doctor for meteorism, presented at the Emergency Room (ER) with persistent constipation for the last six days, associated with nausea and food vomiting within the last 24 hours. Starting on the third day with constipation, the patient also had diffuse, colicky abdominal pain. Upon arrival at the ER, urgent blood tests and standing abdominal x-rays were ordered. Blood tests found leukocytosis at 19,110 x 109/l with predominant neutrophils (74.6%), and no other changes in blood cell counts, renal function, or ions. Abdominal x-rays revealed colonic air-fluid levels; this finding prompted an abdominal CT scan, which showed a large fecal mass at the sigmoid colon with retrograde dilated colonic loops.
The patient was then taken to the observation area, where cleansing enemas and oral lactulose were administered, which failed to resolve the clinical presentation. Attempts to facilitate fecal transit using glycerin enemas were unsuccessful. Following a joint assessment with surgery, an attempt at endoscopic fecalith removal was decided upon. Based on our experience with Coca-Cola® for the management of gastric phytobezoar, as well as the experience reported by other sites, we chose to personally purchase this drink and give it to our patient.
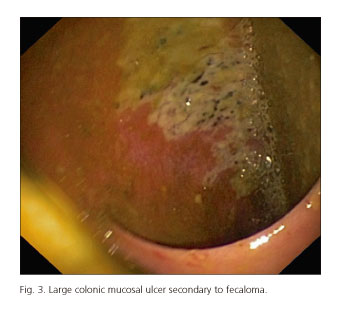
After carefully discussing potential risks with our patient, we performed a colonoscopy using low insufflation pressure to prevent complications, and found the fecaloma. We then proceeded to inject Coca-Cola® within the fecaloma using a sclerosing needle, and then washed the fecaloma surface also with Coca-Cola® with a total volume 500 ml (Figs. 1 and 2). After a few minutes we started to fragment the fecalith, the consistency of which had been notably decreased by the Coca-Cola®, using a polypectomy snare. Following fecalith removal and cleansing, a dilated colonic loop with hyperemic mucosa and a large fibrin-covered ulcer was seen, reflecting ischemic injury on the colonic wall (Fig. 3). Following fecal disimpaction the patient's bowel transit returned to normal, and she was discharged with no complications at 24 hours after the endoscopic procedure.


Discussion
The use of Coca-Cola® for gastric washes in the management of phytobezoars is well established, with a 90% dissolution rate either alone or in combination with subsequent endoscopic fragmentation (4). Phytobezoar composition, including cellulose, lignin, and tannins from fruit and vegetables, is particularly responsive to Coca-Cola®. Although poorly understood, the dissolving power of this drink is mediated by its acidity (5) and the mucolytic effect of NaHCO3, as enhanced by CO2 bubbles (6). Since fecaliths are partly composed of these same substances, the use of Coca-Cola® might well be warranted against them. The management of fecal impaction responsible for intestinal obstruction is usually based on conservative measures. Digital fragmentation of rectal fecalomas, followed by enemas and then oral laxatives, allows most cases to be resolved. However, when such measures fail, surgery may be needed, given the potential complications (ulceration, bleeding, colon perforation) that may arise and their high death rates. A prior step to surgery is using endoscopy to break up the fecaloma with a polypectomy snare (7). In our case, injecting Coca-Cola® into and pouring Coca-Cola® all over the fecaloma eased endoscopic fragmentation and facilitated remission, thus avoiding a mandatory surgical procedure not exempt from serious complications. Our case and the case recently reported by Lee JJ and Kim JW (8) represent the first two reports where Coca-Cola® helped solve colonic obstruction secondary to fecaloma, and might well prompt further studies in order to research the mechanism of action and confirm our findings.
References
1. Longo DL, Fauci AS, Kasper DL, et al. Harrison's principles of internal medicine. 18th edition. McGraw Hill Professional; 2011. [ Links ]
2. Feldman M, Friedman LS, Brandt LJ. Sleisenger and Fordtran's gastrointestinal and liver disease: Pathophysiology/diagnosis/management. 9th edition. Saunders Elsevier; 2010. [ Links ]
3. Corban C, Sommers T, Sengupta N, et al. Fecal impaction in the Emergency Department: An analysis of frequency and associated charges in 2011. J Clin Gastroenterol 2015;50(7):572-7. E-pub ahead of print. DOI: 10.1097/MCG.0000000000000458. [ Links ]
4. Ladas SD, Kamberoglou D, Karamanolis G, et al. Systematic review: Coca-Cola can effectively dissolve gastric phytobezoars as a first-line treatment. Aliment Pharmacol Ther 2013; 37(2):169-73. DOI: 10.1111/apt.12141. [ Links ]
5. Mc CR, Greenberg G, Baron J. Duodenal pH in health and duodenal ulcer disease: Effect of meal, Coca-Cola, smoking and cimetidine. Gut 1984;25:386-92. DOI: 10.1136/gut.25.4.386. [ Links ]
6. Ladas S, Triantafyllou K, Tzathas C, et al. Gastric phytobezoars may be treated by nasogastric Coca-Cola lavage. Eur J Gastroenterol Hepatol 2002;14:801-3. DOI: 10.1097/00042737-200207000-00017. [ Links ]
7. Hussain ZH, Whitehead DA, Lacy BE. Fecal impaction. Curr Gastroenterol Rep 2014;16(9):404. DOI: 10.1007/s11894-014-0404-2. [ Links ]
8. Lee JJ, Kim JW. Successful removal of hard sigmoid fecaloma using endoscopic cola injection. Korean J Gastroenterol 2015;66(1):46-9 DOI: 10.4166/kjg.2015.66.1.46. [ Links ]
![]() Correspondence:
Correspondence:
Guillermo Ontanilla Clavijo.
Department of Clinical Management of Digestive Diseases.
Hospital Universitario Virgen del Rocío.
Av. Manuel Siurot, s/n.
41013 Sevilla, Spain
e-mail: g.ontanilla.clavijo@gmail.com
Received: 10-02-2015
Accepted: 06-05-2016
