










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 n.6 Madrid Jun. 2017
https://dx.doi.org/10.17235/reed.2017.4597/2016
LETTERS TO THE EDITOR
Atraumatic splenic rupture as a complication of acute exacerbation of chronic pancreatitis, an unusual disease
Rotura esplénica atraumática como complicación de pancreatitis crónica reagudizada, un fenómeno poco frecuente
Key words: Splenic rupture. Pancreatitis. Pseudocyst.
Palabras clave: Rotura esplénica. Pancreatitis. Pseudoquiste.
Dear Editor,
Atraumatic splenic rupture is a rare though serious complication of chronic pancreatitis. Approximately 11% of cases are associated with neighboring inflammatory processes.
Case report
A 48-year-old male patient with a history of chronic calcifying pancreatitis with frequent flare-ups of alcoholic origin presented with progressively increasing severe epigastric pain radiating to the back in a belt-like fashion following the ingestion of large amounts of alcohol.
Physical examination revealed a pale, sweaty patient with tachycardia and abdominal epigastric and bilateral hypochondrial tenderness. Lab results included hemoglobin at 7.8 g/dl and hematocrit at 23.5%. Amylase was also increased (338 U/l).
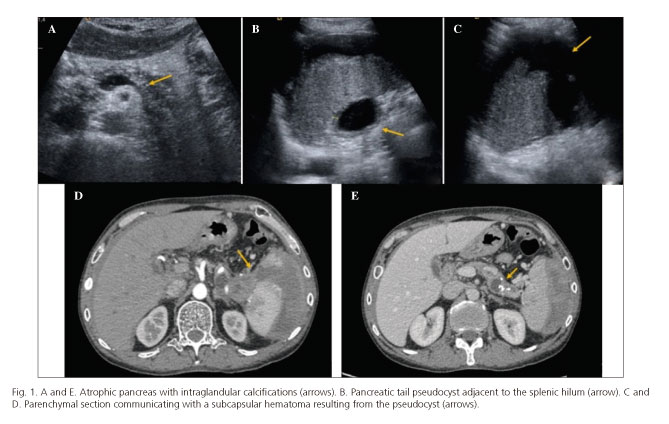
An abdominal ultrasound and contrast-enhanced computed tomography (CT) scan obtained in the late arterial phase and portal phase revealed an atrophic pancreas with disperse calcifications (Fig. 1A and E), as well as a pseudocyst at the splenic hilum (Fig. 1B), which extended across the visceral aspect towards the splenic parenchyma. This resulted in a splenic section communicating with a large subcapsular hematoma (Fig. 1C and D).
The patient underwent a CT-guided puncture draining of the perisplenic hematoma with a favorable outcome.
Discussion
The spleen is anatomically located near the tail of the pancreas, which partly accounts for the pathophysiology of splenic complications most commonly associated with chronic pancreatitis: pseudocysts, subcapsular hematoma, and rupture (1,2).
Among such complications, splenic rupture is rare (0.1-0.5%) (3), and is associated with local inflammatory processes in up to 11% of cases (4).
Initial treatment includes conservative management, percutaneous drainage (indicated for patients ineligible for surgery), and surgery (distal pancreatectomy and splenectomy), which represents a definitive therapy albeit with a high complication rate (5).
To conclude, diagnosing a splenic rupture in the absence of trauma is challenging, with a high index of suspicion being required in cases with pancreatitis.
Elena Moya-Sánchez and Antonio Medina-Benítez
Department of Radiodiagnosis. Complejo Hospitalario Universitario de Granada.
Granada, Spain
References
1. Hernani BL, Silva PC, Nishio RT, et al. Acute pancreatitis complicated with splenic rupture: A case report. World J Gastrointest Surg 2015;7:219-22. DOI: 10.4240/wjgs.v7.i9.219. [ Links ]
2. Sharada S, Olakkengil S, Rozario AP. Occult splenic rupture in a case of chronic calcific pancreatitis with a brief review of literature. Int J Surg Case Rep 2015;14:95-7. DOI: 10.1016/j.ijscr.2015.06.015. [ Links ]
3. Gedik E, Girgin S, Aldemir M, et al. Non-traumatic splenic rupture: Report of seven cases and review of the literature. World J Gastroenterol 2008;14:6711-6. DOI: 10.3748/wjg.14.6711. [ Links ]
4. Renzulli P, Hostettler A, Schoepfer AM, et al. Systematic review of atraumatic splenic rupture. Br J Surg 2009;96:1114-21. DOI: 10.1002/bjs.6737. [ Links ]
5. Heider R, Behrns KE. Pancreatic pseudocysts complicated by splenic parenchymal involvement: Results of operative and percutaneous management. Pancreas 2001;23:20-5. DOI: 10.1097/00006676-200107000-00003. [ Links ]
