










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 no.8 Madrid ago. 2017
DOI: 10.17235/reed.2017.5143/2017
EDITORIAL
The complexity of evaluating and increasing adherence in inflammatory bowel disease
Petra Weimers, Johan Burisch and Pia Munkholm
Department of Gastroenterology. North Zealand University Hospital. Frederikssund, Denmark
Inflammatory bowel diseases (IBDs), due to their chronic and progressive nature, require lifelong treatment to relief and/or prevent inflammation and symptoms, obtaining mucosal healing at best. Therefore, adherence to treatment is an essential topic to address when treating patients with IBD (1). Nonetheless, adherence remains a common and complex issue in IBD care. Patient characteristics such as young age, male sex, and employment have been previously verified as potential predictors of non-adherence (2,3). Additionally, evaluating adherence is in itself a challenge since both accurate and easy-to-use screening tools, as well as golden standards, are lacking.
The current study by De Castro et al., published in this issue of The Spanish Journal of Gastroenterology (4), highlights the problem of how to assess adherence. The authors compared a self-administered scale (Medication Adherence Scale [MMAS-8]) with a medication possession ratio (MPR), and investigated potential predictors of nonadherence using the Beliefs about Medication Questionnaire (BMQ) in 203 IBD patients in clinical remission. More than one third of patients (37%) were considered to be nonadherent by the MPR (golden standard), but less than one fourth (22%) by the MMAS-8, with 15% of patients being incorrectly identified as adherent. However, De Castro et al. (4) found a positive correlation between MPR values and MMAS-8 scores, but only for two drug classes. These findings support the previous conclusions of Kane et al. (5), that the use of MMAS-8 is limited and only significantly correlated to MPR for specific drug classes.
By investigating adherence, patient characteristics, and patient beliefs about medicine, De Castro et al. (4) found that young age, eating alone, missing scheduled medical appointments, and high levels of concern about IBD medication were associated with nonadherence as measured by MMAS-8.
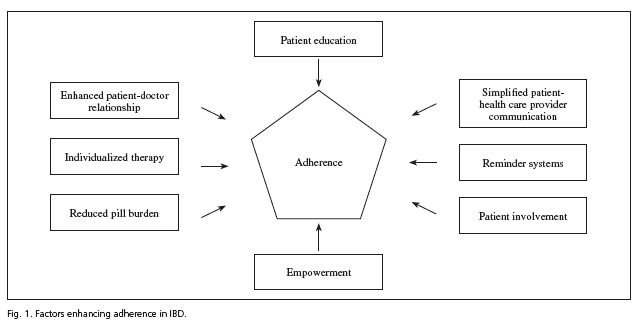
These findings illustrate the lack of a reliable adherence questionnaire, as well as the need for clinical innovations to improve medical adherence in IBD patients. In order to enhance adherence, it is important to identify the reason (voluntary or involuntary) for nonadherence (6). Behavioral interventions, such as reduced pill burden and simplified dosing regimens (once or twice daily), appear to have a positive impact on adherence (6-9). Furthermore, reminder systems, both traditional, such as pill boxes, and novel, such as e-mail and telephone alarms, have been suggested to be useful behavioral interventions for patients with involuntary adherence issues (6). Good patient-doctor relationship, as well as optimized patient education and information, is of great importance for both accidental and volitional nonadherent IBD patients (6,10).
Despite the positive findings of previous studies on educational and behavioral approaches, nonadherence is still a complex problem in IBD patients. Multicomponent interventions, combining educational and behavioral approaches, suggest a more positive effect on adherence than either approach alone (11). During the last decade several innovative telemedicine devices, with combined approaches, have been developed to increase disease understanding, patient involvement and adherence in adult and pediatric IBD patients (12-14).
The first international randomized, controlled eHealth trial including IBD patients showed that the use of a web-program, Constant Care, not only increased adherence (OR 13.83) and quality of life (OR 1.57) but also empowerment for self-initiated treatment and reduced healthcare costs (12). The web-program has since been evaluated with positive results in several trials of both adult and pediatric IBD patients (15-17). Constant Care includes an educational module, an individualized feedback system, and a communication module. The web program's feedback system consequently provides patients with an individualized therapy option (based on patient-reported symptom severity), thereby directly involving patients in the treatment of their disease. The feedback system empowers patients to self-initiate treatment, and they also have the possibility of contacting their doctor directly through the communication module (12,18). The role of increased patient empowerment and involvement in the monitoring and treatment of their disease seems to be vital in achieving increased treatment adherence. Similar telemedicine devices, with integrated disease monitoring, e-learning and communication modules, have been recently developed (19), and patient involvement seems to be key in obtaining sufficient patient adherence (20).
The study by De Castro et al. (4) has contributed important knowledge regarding the complexity of adherence and how to assess it properly. Several different adherence-enhancing factors have been proposed during the last couple of years (Fig. 1). Future studies will need to focus on the development of a reliable adherence questionnaire, and on how to increase patient involvement, education, and information in order to obtain improved adherence in IBD patients.
References
1. Kane S, Huo D, Aikens J, et al. Medication nonadherence and the outcomes of patients with quiescent ulcerative colitis. Am J Med 2003;114(1):39-43. DOI: 10.1016/S0002-9343(02)01383-9. [ Links ]
2. Severs M, Zuithoff PNPA, Mangen M-JJ, et al. Assessing self-reported medication adherence in inflammatory bowel disease. Inflamm Bowel Dis 2016;22(9):2158-64. DOI: 10.1097/MIB.0000000000000853. [ Links ]
3. Kane S V., Cohen RD, Aikens JE, et al. Prevalence of nonadherence with maintenance mesalamine in quiescent ulcerative colitis. Am J Gastroenterol 2001;96(10):2929-33. DOI: 10.1111/j.1572-0241.2001.04683.x. [ Links ]
4. De Castro M-L, Sanromán L, Martín A, et al. Assessing medication adherence in Inflammatory Bowel Diseases. A comparison between a self-administered scale and a pharmacy refill index. Spanish J Gastroenterol 2017;109(8):542-51. DOI: 10.17235/reed.2017.5137/2017. [ Links ]
5. Kane S, Becker B, Scott Harmsen W, et al. Use of a screening tool to determine nonadherent behavior in inflammatory bowel disease. Am J Gastroenterol 2012;107(10). DOI: 10.1038/ajg.2011.317. [ Links ]
6. Bermejo F, López-San Román A, Algaba A, et al. Factors that modify therapy adherence in patients with inflammatory bowel disease. J Crohn's Colitis 2010;4:422-6. DOI: 10.1016/j.crohns.2010.01.005. [ Links ]
7. Kane SV. Systematic review: adherence issues in the treatment of ulcerative colitis. Aliment Pharmacol Ther 2006;23(5):577-85. DOI: 10.1111/j.1365-2036.2006.02809.x. [ Links ]
8. Greenberg RN. Overview of patient compliance with medication dosing: a literature review. Clin Ther 1984;6(5):592-9. [ Links ]
9. Algaba A, Guerra I, García García de Paredes A, et al. What is the real-life maintenance mesalazine dose in ulcerative colitis? Rev Española Enfermedades Dig 2016;109(2):114-21. DOI: 10.17235/reed.2016.4620/2016. [ Links ]
10. Robinson A. Review article: improving adherence to medication in patients with inflammatory bowel disease. Aliment Pharmacol Ther 2008;27:9-14. DOI: 10.1111/j.1365-2036.2008.03604.x. [ Links ]
11. Greenley RN, Kunz JH, Walter J, et al. Practical strategies for enhancing adherence to treatment regimen in inflammatory bowel disease. Inflamm Bowel Dis 2013;19(7):1534-45. DOI: 10.1097/MIB.0b013e3182813482. [ Links ]
12. Elkjaer M, Shuhaibar M, Burisch J, et al. E-health empowers patients with ulcerative colitis: a randomised controlled trial of the web-guided "Constant-care" approach. Gut 2010;59(12):1652-61. DOI: 10.1136/gut.2010.220160. [ Links ]
13. Cross RK, Cheevers N, Rustgi A, et al. A Randomized, Controlled Trial of Home Telemanagement in Patients with Ulcerative Colitis (UC HAT). Inflamm Bowel Dis 2012;18(6):1018. DOI: 10.1002/ibd.21795. [ Links ]
14. Hommel KA, Hente E, Herzer M, et al. Telehealth behavioral treatment for medication nonadherence: a pilot and feasibility study. Eur J Gastroenterol Hepatol 2013;25(4):469-73. DOI: 10.1097/MEG.0b013e32835c2a1b. [ Links ]
15. Carlsen K, Jakobsen C, Houen G, et al. Self-managed eHealth disease monitoring in children and adolescents with inflammatory bowel disease. Inflamm Bowel Dis 2017;23(3):357-65. DOI: 10.1097/MIB.0000000000001026. [ Links ]
16. Pedersen N, Elkjaer M, Duricova D, et al. eHealth: individualisation of infliximab treatment and disease course via a self-managed web-based solution in Crohn's disease. Aliment Pharmacol Ther 2012;36(9):840-9. DOI: 10.1111/apt.12043. [ Links ]
17. Pedersen N, Thielsen P, Martinsen L, et al. eHealth: individualization of mesalazine treatment through a self-managed web-based solution in mild-to-moderate ulcerative colitis. Inflamm Bowel Dis 2014;20(12):2276-85. DOI: 10.1097/MIB.0000000000000199. [ Links ]
18. Elkjaer M, Burisch J, Avnstrøm S, et al. Development of a Web-based concept for patients with ulcerative colitis and 5-aminosalicylic acid treatment. Eur J Gastroenterol Hepatol 2009;22(6):1. DOI: 10.1097/MEG.0b013e32832e0a18. [ Links ]
19. de Jong M, van der Meulen-de Jong A, Romberg-Camps M, et al. Development and Feasibility Study of a Telemedicine Tool for All Patients with IBD. Inflamm Bowel Dis 2017;23(4):485-93. DOI: 10.1097/MIB.0000000000001034. [ Links ]
20. Bager P, Julsgaard M, Vestergaard T, et al. Scandinavian Journal of Gastroenterology Adherence and quality of care in IBD Adherence and quality of care in IBD. Scand J Gastroenterol 2016;5111:1326-31. DOI: 10.1080/00365521.2016.1195870. [ Links ]
