










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 no.8 Madrid ago. 2017
https://dx.doi.org/10.17235/reed.2017.4633/2016
LETTERS TO THE EDITOR
The clinical challenge of chronic Q fever with isolated liver involvement
Key words: Granulomatous hepatitis. Chronic Q fever.
Dear Editor,
Chronic Q fever is defined as an infection by Coxiella burnetii (C. burnetii) that lasts for six months or more (1). It occurs in 1-5% of individuals infected with this agent and develops over a period of months to years after the acute infection (2). Cases of hepatic involvement are rare (3).
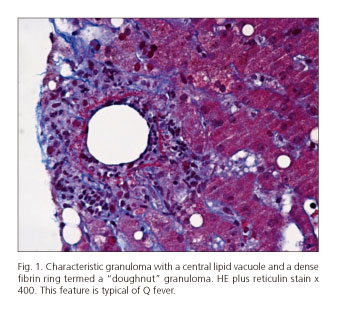
We report the case of a 38-year-old male with persistent elevation of aminotransferases and gamma-glutamyltransferase, two to three times the upper normal limit, with an evolution of ten years. The standard tests for liver diseases were negative. Due to the diagnostic uncertainty a liver biopsy was performed. The analysis described the following relevant findings: expansion of some portal spaces by confluent epithelioid granulomas (Ziehl-Neelsen, PAS and PAS-D negative) (Fig. 1). Further studies addressed the potential causes of granulomatous liver disease. A positive reaction to the anti-C. burnetii antibody was observed, and the infection was subsequently confirmed by the polymerase chain reaction (PCR). The patient started on empirical treatment with doxycycline 200 mg/day and the subsequent liver tests were normal.
Chronic Q fever with only hepatic involvement is rare, and a high clinical suspicion and knowledge of the appropriate diagnostic methods and their limitations is required, particularly in the absence of symptoms. Patients with chronic Q fever are often ill for more than one year before a diagnosis is made (4). Serology is the most commonly used diagnostic tool. Indirect immunofluorescence is sensitive and specific, and it is the method of choice in most countries. In addition, a sample of whole blood can be tested by PCR to determine if a patient has Q fever. However, other causes of chronically abnormal liver tests should be excluded, especially when there is an epidemiological history of a possible exposure to C. burnetii, thus, reducing the probability of future complications.
Armando Peixoto, Pedro Pereira and Guilherme Macedo
Gastroenterology Department. Centro Hospitalar de São João.
Faculty of Medicine. University of Porto. Porto, Portugal
References
1. Raoult D, Marrie T. Q fever. Clin Infect Dis 1995;20(3):489. DOI: 10.1093/clinids/20.3.489. [ Links ]
2. Million M, Walter G, Bardin N, et al. Immunoglobulin G anticardiolipin antibodies and progression to Q fever endocarditis. Clin Infect Dis 2013;57(1):57-64. DOI: 10.1093/cid/cit191. [ Links ]
3. Marrie TJ, Raoult D. Q fever - A review and issues for the next century. Int J Antimicrob Agents 1997;8(3):145. DOI: 10.1016/S0924-8579(96)00369-X. [ Links ]
4. Harris RJ, Storm PA, Lloyd A, et al. Long-term persistence of Coxiella burnetii in the host after primary Q fever. Epidemiol Infect 2000;124(3):543-9. DOI: 10.1017/S0950268899003763. [ Links ]
