










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 n.10 Madrid Oct. 2017
https://dx.doi.org/10.17235/reed.2017.4717/2016
ORIGINAL PAPERS
Direct percutaneous endoscopic jejunostomy using single-balloon enteroscopy without fluoroscopy: a case series
Carlos Bernardes1, Rolando Pinho2, Adélia Rodrigues2, Luísa Proença2 and João Carvalho2
1Department of Gastroenterology. Centro Hospitalar de Lisboa Central. Lisboa, Portugal.
2Department of Gastroenterology and Hepatology. Centro Hospitalar de Vila Nova de Gaia/Espinho. Vila Nova de Gaia, Portugal
ABSTRACT
Background: Direct percutaneous endoscopic jejunostomy (DPEJ) is a useful method to provide enteral nutrition to individuals when gastric feeding is not possible or contraindicated. The aim of this study was to analyze the efficacy and safety of DPEJ tube placement with the Gauderer-Ponsky technique by the pull method, using single-balloon enteroscopy (SBE) without fluoroscopy.
Methods: This is a retrospective analysis of patients undergoing SBE for DPEJ placement in a referral hospital between January 2010 and March 2016. Technical success, clinical success and procedure related complications were recorded.
Results: Twenty-three patients were included (17 males, median age 71 years, range 37-93 years). The most frequent indications for DPEJ were gastroesophageal cancer (n = 10) and neurological disease (n = 8). Eighty-seven percent of the patients had a contraindication to percutaneous endoscopic gastrostomy (PEG) and PEG was unsuccessful in the remaining patients. The technical success rate was 83% (19/23), transillumination was not possible in three patients and an accidental exteriorization of the bumper resulting in a jejunal perforation occurred in one patient. The clinical success was 100% (19/19). The median follow-up was five months (range 1-35 months). Apart from the case of jejunal perforation and the two cases of accidental exteriorization, there were no other complications during follow-up. The 6-month survival was 65.8% and the 1-year survival was 49.3%.
Conclusion: DPEJ can be carried out successfully via SBE without fluoroscopy with a low rate of significant adverse events. Although, leaving the overtube in place during the bumper pulling can be useful for distal jejunal loops, it can be safely removed in proximal loops to minimize complications.
Key words: Jejunostomy. Direct percutaneous endoscopic jejunostomy. Enteroscopy. Single balloon enteroscopy. Enteral feeding.
Introduction
Enteral feeding via a percutaneously placed device provides adequate nutritional support for individuals who are unable to maintain oral intake (1,2). Gastric feeding with a percutaneous endoscopic gastrostomy (PEG) is usually the preferred method for long term enteral nutrition. However, a jejunal route is required for patients in which PEG placement is not possible as well as those with gastroparesis, gastric neoplasia, risk of aspiration or previous gastroesophageal surgery (3-5). Direct percutaneous endoscopic jejunostomy (DPEJ) has proven to be more effective and secure than PEG with a jejunal extension tube (PEG-J) (6,7). This procedure may be carried out with adult or pediatric endoscopes via a percutaneous gastrostomy orifice or with push enteroscopes or balloon-assisted enteroscopes. Several techniques have been described, such as the "T" pexies triangulation system, magnetic jejunal anchors, and overtube maintenance during bumper pulling or with fluoroscopy guidance (8-15). In spite of all different approaches, DPEJ is considered to be a technically difficult procedure with success rates ranging from 68% to 100% (3,16). We present our experience of single-balloon enteroscopy (SBE)-assisted DPEJ placement without fluoroscopy and maintaining the overtube during the pull maneuver only for distal jejunal loops.
Methods
A retrospective, descriptive study was conducted that involved all patients who underwent DPEJ at the Centro Hospitalar de Vila Nova de Gaia/Espinho in Portugal, between January 2010 and February 2016. Data regarding patient demographics, indications for enteral feeding and DPEJ, procedure-related complications and adverse events were reviewed until removal of the DPEJ or patient death. Technical success was defined as an uneventful DPEJ placement. Clinical success was defined as the effective use of the DPEJ tube for feeding patients in whom technical success was achieved. Informed consent was obtained for every examination. Statistical analysis included descriptive statistics and survival analysis using the Kaplan-Meier method.
All patients were referred due to a contraindication for gastric feeding or following failed PEG insertion. SBE was carried out using the SIF-Q180 enteroscope (Olympus, Tokyo, Japan), a 200 cm long enteroscope with a 2.8 mm working channel. The enteroscope was used with a 140 cm long silicone overtube ST-SB1 (Olympus, Tokyo, Japan). All patients were under deep propofol sedation and received a 1-g dose of intravenous ceftriaxone 30 minutes before the examination. The SBE was advanced to the jejunum and, according to the Gauderer-Ponsky technique, a loop was selected via transillumination and finger indentation. After applying local antiseptic, a 40-mm 21-G needle was used for lidocaine infiltration and jejunal puncture and fixation. For fixation, the needle was grasped with a snare during skin incision, gastrostomy catheter puncture and string advancement. The needle was then withdrawn while the string was grasped with foreign body forceps. The maintenance or removal of the overtube during PEJ-bumper pulling (20 Fr, US Endoscopy, Mentor, OH, USA) was performed depending on the depth of insertion into the jejunum. Following uneventful placement of the device, an enteral diet was started on the same day. PEJ tubes were substituted by balloon replacement gastrostomy tubes (PEG-18-BRT-S, Cook Medical Inc., Bloomington, USA) after one year of follow-up or when required. Balloon replacement tubes were subsequently substituted at three month intervals.
Results
Twenty-three patients (17 males and six females, with a median age of 71 years, range 37-93 years) underwent SBE-assisted DPEJ (Table 1). Ten patients required artificial enteral feeding due to gastroesophageal neoplasia (seven with gastric and three with esophageal adenocarcinoma). Eight patients had neurological diseases that caused dysphagia, three had head and neck neoplasia, one had severe refractory gastric stasis and one had necrotizing pancreatitis. Three patients had a previous attempt at PEG insertion which was unsuccessful as no transillumination area was identified during the procedure. The remaining 20 patients underwent DPEJ due to PEG contraindication; this included post-partial gastrectomy status (n = 10), unresectable gastric cancer causing gastric outlet obstruction (n = 7), severe gastroparesis (n = 1), necrotizing pancreatitis (n = 1) and refractory gastric ulcers (n = 1). The technical success rate was 83% (19/23). Identification of a specific jejunal loop via transillumination and finger indentation was not possible in three patients, two of whom were obese (body mass index [BMI] > 30 kg/m2). However, DPEJ placement was accomplished in all patients with previously failed PEG insertion. In one patient, an overtube-related complication occurred during the pulling maneuver: the PEJ bumper became fixed at the tip of the overtube. Gentle traction to release the bumper was attempted, resulting in an accidental exteriorization of the bumper from the overtube and through the jejunal wall that lead to a perforation. The patient underwent surgery. Following this event, the overtube was removed before the pulling maneuver and a proximal jejunal loop was targeted which was left in place only for distal loops. The clinical success rate was 100% (19/19) as all the devices were properly used for enteral feeding. The median follow-up time was five months (range 1-35 months). Two cases of accidental exteriorization of the PEJ-bumper during the follow-up period were recorded, both male patients with a diagnosis of esophageal adenocarcinoma. One occurred thirteen months after DPEJ insertion (this patient died a few days after this event due to oncological disease) and the other case occurred ten months after the procedure.
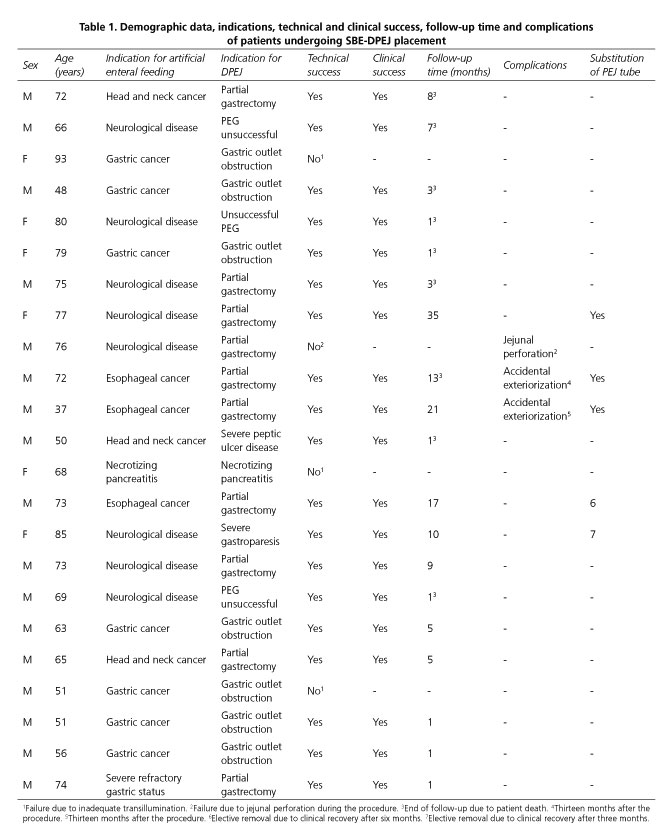
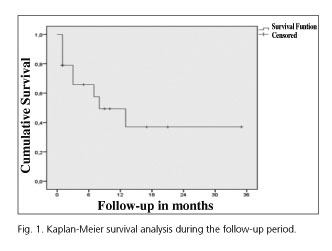
There have been no other short or long-term adverse events during the follow-up period. Among the patients with a technical and clinical success, the 6-month survival was 65.8% and the 1-year survival was 49.3%.
Substitution of the PEJ tube for the balloon tube replacement and further balloon tube replacements were performed uneventfully in three patients, on an outpatient basis without endoscopic control. PEJ was electively removed due to clinical recovery in two patients, one with neurological impairment and another with esophageal adenocarcinoma (after three and six months of follow-up, respectively).
Two cases of accidental removal occurred. Partial closure of the fistula occurred in one case and the PEJ replacement required an ultrasound-assisted technique. A 14 Fr catheter was inserted through the tract and its intraluminal position was confirmed using ultrasound. Subsequently, a guide-wire was placed, the PEJ stoma was enlarged via a scalpel incision and the new balloon tube was finally introduced under ultrasound guidance (20).
Discussion
Although DPEJ placement was first performed almost 30 years ago, it still is a challenging technique with variable failure rates. In fact, the largest published study comprised 307 patients with a success rate of only 68% (3). Thus, different approaches have been adopted to overcome the procedure-related obstacles.
Balloon-assisted enteroscopy allows an easier and deeper intubation of the small bowel and plays an important role in locating an adequate site of transillumination. Several researchers have achieved successful results using double-balloon enteroscopy (DBE), with a relatively low complication rate (6,10,17). Aktas et al. reported their experience in 12 patients undergoing DPEJ insertion, with a technical success rate of 92% (11). To our knowledge this is the second and the largest case series using SBE. We achieved a technical success rate of 83%, mainly due to the inability to identify a transillumination area, which occurred in three cases. As previously noted, two of these patients were obese, a condition which accounts for a higher failure rate (3,18). An analysis carried out by Mackenzie et al. demonstrated the impact of BMI on the effectiveness of DPEJ insertion. The authors reported an overall success rate of 81% in 80 DPEJ placement attempts, reporting a 96% (23/24) and 81% (25/31) success rate for underweight (BMI < 18.5 kg/m2) and normal weight (BMI 18.5-24.9 kg/m2) patients, respectively.
The technical success rate was only 60% (6/10) in obese individuals (18). One of the most critical steps of this procedure is the detection of an adequate jejunal loop to puncture, and it is difficult to obtain transillumination and finger indentation in patients with a thick abdominal wall. In fact, other studies have shown that abdominal wall thickness measured by a pre-procedure abdominal computed tomography (CT) scan can help to predict outcome in these individuals, and the DPEJ success rate in patients with an abdominal wall thickness greater than 3 cm was only 39% (19).
In order to improve yield and to minimize complications, numerous techniques and approaches have been described for DPEJ placement. The anatomical distribution and peristalsis of the jejunum results in difficulties for a proper insertion of the device and increases the risk of adverse events. Alberta-de-las-Parras et al. presented a pediatric case with DPEJ placement using a pediatric endoscope via a previous gastrostomy orifice. A triangulation "T" pexies system was used to fix the jejunal loop against the abdominal wall which allowed a direct introduction of the balloon tube and minimized the risk of loop displacement during the procedure (12). Similarly, magnetic anchors were tested in porcine models to enable jejunal loop fixation and facilitate the execution of the DPEJ via DBE under more stable and safer circumstances (13). For this purpose, the technique described here includes grasping the needle with a snare after puncture of the intestinal loop which ensured its anchorage and avoided needle exteriorization. Velázquez-Avinã et al. used fluoroscopic guidance to confirm the puncture site, and recommended leaving the overtube in place while the string is removed with the scope and then it is reintroduced with the PEJ-bumper (14). In our experience, fluoroscopy is not necessary as there were no complications during or after puncture of the selected loop when transillumination and finger indentation were achieved. However, this method could be helpful in difficult cases, such as obese patients, as discussed previously. With regard to maintaining the overtube in place during the pulling maneuver, we agree that it can be useful for DPEJ placement in a distal position; however, we consider it unnecessary for proximal jejunal loops, as bumper pulling and endoscopic confirmation of the final position of the bumper may be easily and safely performed (20). Removal of the overtube may reduce the risk of adverse events, such as bowel perforation, which was one of the two unique complications observed in our series.
Unintentional exteriorization of the PEJ tube may occur and, as with PEG tubes, closure of the enterocutaneous fistula usually develops within the first 24 hours. Timely replacement of the PEJ tube should be attempted in these patients. In certain cases, salvage rescue techniques to save the PEJ tract may be required, such as an ultrasound-assisted technique of PEJ replacement (21) and/or dilatation of the PEJ tract.
In conclusion, DPEJ is a useful approach for patients who require enteral feeding and are not suitable for PEG placement. This procedure can be effectively and safely carried out via SBE without fluoroscopy in the vast majority of patients, leaving the overtube during bumper advancement only for distal jejunal loops. Since the technical success rate is lower among obese individuals, prior CT scan evaluation and fluoroscopic assistance could be helpful in these cases.
References
1. Di Sario JA. Endoscopic approaches to enteral nutritional support. Best Pract Res Clin Gastroenterol 2006;20(3):605-30. DOI: 10.1016/j.bpg.2006.02.002. [ Links ]
2. Zhu Y, Shi L, Tang H, et al. Current considerations in direct percutaneous endoscopic jejunostomy. Can J Gastroenterol 2012;26(2):92-6. DOI: 10.1155/2012/319843. [ Links ]
3. Maple JT, Petersen BT, Baron TH, et al. Direct percutaneous endoscopic jejunostomy: Outcomes in 307 consecutive attempts. Am J Gastroenterol 2005;100:2681-8. DOI: 10.1111/j.1572-0241.2005.00334.x. [ Links ]
4. Auvin S, Michaud L, Guimber D, et al. Percutaneous endoscopic jejunostomy for decompression in an infant with short-bowel syndrome. Endoscopy 2000;34(3):240. [ Links ]
5. Panagiotakis P, Di Sario J, Hilden K, et al. DPEJ tube placement prevents aspiration pneumonia in high-risk patients. Nutr Clin Pract 2008;23(2):172-5. DOI: 10.1177/0884533608314537. [ Links ]
6. Lim AH, Schoeman MN, Nguyen NQ. Long-term outcomes of direct percutaneous endoscopic jejunostomy: A 10-year cohort. Endosc Int Open 2015;3(6):E610-4. DOI: 10.1055/s-0034-1392806. [ Links ]
7. Delegge MH, Ginsberg G, McClave S, et al. Randomized prospective comparison of direct percutaneous endoscopic jejunostomy (DPEJ) feeding tube placement versus percutaneous endoscopic gastrostomy feeding tube placement with jejunal extension (PEG-J), for enteral feeding. Gastrointest Endosc 2006;63(5):AB160. DOI: 10.1016/j.gie.2006.03.320. [ Links ]
8. Del Piano M, Ballaré M, Carmagnola S, et al. DPEJ placement in cases of PEG insertion failure. Dig Liver Dis 2008;40(2)140-3. DOI: 10.1016/j.dld.2007.09.012. [ Links ]
9. Shike M, Latkany L, Gerdes H, et al. Direct percutaneous endoscopic jejunostomies for enteral feeding. Gastrointest Endosc 1996;44:536-40. DOI: 10.1016/S0016-5107(96)70005-6. [ Links ]
10. Aktas H, Mensink PB, Kuipers EJ, et al. Single-balloon enteroscopy-assisted direct percutaneous endoscopic jejunostomy. Endoscopy 2012;44(2):210-2. DOI: 10.1055/s-0031-1291442. [ Links ]
11. Despott EJ, Gabe S, Tripoli E, et al. Enteral access by double-balloon enteroscopy: An alternative method of direct percutaneous endoscopic jejunostomy placement. Dig Dis Sci 2011;56(2):494-8. DOI: 10.1007/s10620-010-1306-2. [ Links ]
12. Alberca-de-las-Parras F, Navalón-Rubio M, Egea-Valenzuela J, et al. Direct percutaneous endoscopic jejunostomy in pediatric age with a pexies triangulation system: Report of a case and literature review. Rev Esp Enferm Dig 2015;107(4):240-2. [ Links ]
13. Yano T, Sunada K, Yoshizawa M, et al. New technique for direct percutaneous endoscopic jejunostomy using double balloon endoscopy and magnetic anchors in a porcine model. Dig Endosc 2011;23(2):206. DOI: 10.1111/j.1443-1661.2010.01079.x. [ Links ]
14. Velázques-Aviña J, Beyer R, Díaz-Tobar CP, et al. New method of direct percutaneous endoscopic jejunostomy tube placement using balloon-assisted enteroscopy with fluoroscopy. Dig Endosc 2015;27(3):317-22. DOI: 10.1111/den.12352. [ Links ]
15. Shetzline MA, Suhocki PV, Workman MJ. Direct percutaneous endoscopic jejunostomy with small bowel enteroscopy and fluoroscopy. Gastrointest Endosc 2001;53(6):633-8. DOI: 10.1067/mge.2001.114420. [ Links ]
16. Barrera R, Schattner M, Nygard S, et al. Outcome of direct percutaneous endoscopic jejunostomy tube placement for nutritional support in critically ill, mechanically ventilated patients. J Crit Care 2001;16(4):178-81. DOI: 10.1053/jcrc.2001.30667. [ Links ]
17. Al-Bawardy B, Gorospe EC, Alexander JA, et al. Outcomes of double-balloon enteroscopy-assisted direct percutaneous endoscopicjejunostomy tube placement. Endoscopy 2016;48(6):552-6. DOI: 10.1055/s-0042-101853. [ Links ]
18. Mackenzie SH, Haslem D, Hilden K, et al. Success rate of direct percutaneous endoscopic jejunostomy in patients who are obese. Gastrointest Endosc 2008;67(2):265-9. DOI: 10.1016/j.gie.2007.06.041. [ Links ]
19. Maple JT, Petersen BT, Baron TH, et al. Abdominal CT as a predictor of outcome before attempted direct percutaneous endoscopic jejunostomy. Gastrointest Endosc 2006;63(3):424-30. DOI: 10.1016/j.gie.2005.10.035. [ Links ]
20. Pinho RT, Rodrigues MA, Proença ML. Overtubes and fluoroscopy for direct percutaneous endoscopic jejunostomy: Useful, although not always needful and sometimes harmful. Dig Endosc 2015;27(3):399-400. DOI: 10.1111/den.12426. [ Links ]
21. Ponte A, Pinho R, Fernandes S, et al. Ultrasound-assisted technique for challenging jejunostomy balloon-tube replacements. Rev Esp Enferm Dig 2016;108(10):657-8. [ Links ]
![]() Correspondence:
Correspondence:
Carlos Bernardes.
Department of Gastroenterology.
Centro Hospitalar de Lisboa Central.
Lisboa, Portugal
e-mail: carlosfbernardes@gmail.com
Received: 08-11-2016
Accepted: 31-05-2017
